- Research article
- Open access
- Published: 15 February 2023

The impact of food insecurity on health outcomes: empirical evidence from sub-Saharan African countries
- Sisay Demissew Beyene ORCID: orcid.org/0000-0001-7347-4168 1
BMC Public Health volume 23 , Article number: 338 ( 2023 ) Cite this article
27k Accesses
24 Citations
14 Altmetric
Metrics details
Food insecurity adversely affects human health, which means food security and nutrition are crucial to improving people’s health outcomes. Both food insecurity and health outcomes are the policy and agenda of the 2030 Sustainable Development Goals (SDGs). However, there is a lack of macro-level empirical studies (Macro-level study means studies at the broadest level using variables that represent a given country or the whole population of a country or economy as a whole. For example, if the urban population (% of the total population) of XYZ country is 30%, it is used as a proxy variable to represent represent country's urbanization level. Empirical study implies studies that employ the econometrics method, which is the application of math and statistics.) concerning the relationship between food insecurity and health outcomes in sub-Saharan African (SSA) countries though the region is highly affected by food insecurity and its related health problems. Therefore, this study aims to examine the impact of food insecurity on life expectancy and infant mortality in SSA countries.
The study was conducted for the whole population of 31 sampled SSA countries selected based on data availability. The study uses secondary data collected online from the databases of the United Nations Development Programme (UNDP), the Food and Agricultural Organization (FAO), and the World Bank (WB). The study uses yearly balanced data from 2001 to 2018. This study employs a multicountry panel data analysis and several estimation techniques; it employs Driscoll-Kraay standard errors (DKSE), a generalized method of momentum (GMM), fixed effects (FE), and the Granger causality test.
A 1% increment in people’s prevalence for undernourishment reduces their life expectancy by 0.00348 percentage points (PPs). However, life expectancy rises by 0.00317 PPs with every 1% increase in average dietary energy supply. A 1% rise in the prevalence of undernourishment increases infant mortality by 0.0119 PPs. However, a 1% increment in average dietary energy supply reduces infant mortality by 0.0139 PPs.
Conclusions
Food insecurity harms the health status of SSA countries, but food security impacts in the reverse direction. This implies that to meet SDG 3.2, SSA should ensure food security.
Peer Review reports
Food security is essential to people’s health and well-being [ 1 ]. Further, the World Health Organization (WHO) argues that health is wealth and poor health is an integral part of poverty; governments should actively seek to preserve their people’s lives and reduce the incidence of unnecessary mortality and avoidable illnesses [ 2 ]. However, lack of food is one of the factors which affect health outcomes. Concerning this, the Food Research and Action Center noted that the social determinants of health, such as poverty and food insecurity, are associated with some of the most severe and costly health problems in a nation [ 3 ].
According to the FAO, the International Fund for Agricultural Development (IFAD), and the World Food Programme (WFP), food insecurity is defined as "A situation that exists when people lack secure access to sufficient amounts of safe and nutritious food for normal growth and development and an active and healthy life" ([ 4 ]; p50). It is generally believed that food security and nutrition are crucial to improving human health and development. Studies show that millions of people live in food insecurity, which is one of the main risks to human health. Around one in four people globally (1.9 billion people) were moderately or severely food insecure in 2017 and the greatest numbers were in SSA and South Asia. Around 9.2% of the world's population was severely food insecure in 2018. Food insecurity is highest in SSA countries, where nearly one-third are defined as severely insecure [ 5 ]. Similarly, 11% (820 million) of the world's population was undernourished in 2018, and SSA countries still share a substantial amount [ 5 ]. Even though globally the number of people affected by hunger has been decreasing since 1990, in recent years (especially since 2015) the number of people living in food insecurity has increased. It will be a huge challenge to achieve the SDGs of zero hunger by 2030 [ 6 ]. FAO et al. [ 7 ] projected that one in four individuals in SSA were undernourished in 2017. Moreover, FAO et al. [ 8 ] found that, between 2014 and 2018, the prevalence of undernourishment worsened. Twenty percent of the continent's population, or 256 million people, are undernourished today, of which 239 million are in SSA. Hidden hunger is also one of the most severe types of malnutrition (micronutrient deficiencies). One in three persons suffers from inadequacies related to hidden hunger, which impacts two billion people worldwide [ 9 ]. Similarly, SSA has a high prevalence of hidden hunger [ 10 , 11 ].
An important consequence of food insecurity is that around 9 million people die yearly worldwide due to hunger and hunger-related diseases. This is more than from Acquired Immunodeficiency Syndrome (AIDS), malaria, and tuberculosis combined [ 6 ]. Even though the hunger crisis affects many people of all genders and ages, children are particularly affected in Africa. There are too many malnourished children in Africa, and malnutrition is a major factor in the high infant mortality rates and causes physical and mental development delays and disorders in SSA [ 12 ]. According to UN statistics, chronic malnutrition globally accounts for 165 million stunted or underweight children. Around 75% of these kids are from SSA and South Asia. Forty percent of children in SSA are impacted. In SSA, about 3.2 million children under the age of five dies yearly, which is about half of all deaths in this age group worldwide. Malnutrition is responsible for almost one child under the age of five dying every two minutes worldwide. The child mortality rate in the SSA is among the highest in the world, about one in nine children pass away before the age of five [ 12 ].
In addition to the direct impact of food insecurity on health outcomes, it also indirectly contributes to disordered eating patterns, higher or lower blood cholesterol levels, lower serum albumin, lower hemoglobin, vitamin A levels, and poor physical and mental health [ 13 , 14 , 15 ]. Iodine, iron, and zinc deficiency are the most often identified micronutrient deficiencies across all age groups. A deficiency in vitamin A affects an estimated 190 million pre-schoolers and 19 million pregnant women [ 16 ]. Even though it is frequently noted that hidden hunger mostly affects pregnant women, children, and teenagers, it further affects people’s health at all stages of life [ 17 ].
With the above information, researchers and policymakers should focus on the issue of food insecurity and health status. The SDGs that were developed in 2015 intend to end hunger in 2030 as one of its primary targets. However, a growing number of people live with hunger and food insecurity, leading to millions of deaths. Hence, this study questioned what is the impact of food insecurity on people's health outcomes in SSA countries. In addition, despite the evidence implicating food insecurity and poor health status, there is a lack of macro-level empirical studies concerning the impact of food insecurity on people’s health status in SSA countries, which leads to a knowledge (literature) gap. Therefore, this study aims to examine the impact of food insecurity on life expectancy and infant mortality in SSA countries for the period ranging from 2001–2018 using panel mean regression approaches.
Theoretical and conceptual framework
Structural factors, such as climate, socio-economic, social, and local food availability, affect people’s food security. People’s health condition is impacted by food insecurity through nutritional, mental health, and behavioral channels [ 18 ]. Under the nutritional channel, food insecurity has an impact on total caloric intake, diet quality, and nutritional status [ 19 , 20 , 21 ]. Hunger and undernutrition may develop when food supplies are scarce, and these conditions may potentially lead to wasting, stunting, and immunological deficiencies [ 22 ]. However, food insecurity also negatively influences health due to its effects on obesity, women's disordered eating patterns [ 23 ], and poor diet quality [ 24 ].
Under the mental health channel, Whitaker et al. [ 25 ] noted that food insecurity is related to poor mental health conditions (stress, sadness, and anxiety), which have also been linked to obesity and cardiovascular risk [ 26 ]. The effects of food insecurity on mental health can worsen the health of people who are already sick as well as lead to disease acquisition [ 18 ]. Similarly, the behavioral channel argues that there is a connection between food insecurity and health practices that impact disease management, prevention, and treatment. For example, lack of access to household food might force people to make bad decisions that may raise their risk of sickness, such as relying too heavily on cheap, calorically dense, nutrient-poor meals or participating in risky sexual conduct. In addition, food insecurity and other competing demands for survival are linked to poorer access and adherence to general medical treatment in low-income individuals once they become sick [ 27 , 28 , 29 , 30 ]
Food insecurity increases the likelihood of exposure to HIV and worsens the health of HIV-positive individuals [ 18 ]. Weiser et al. [ 31 ] found that food insecurity increases the likelihood of unsafe sexual activities, aggravating the spread of HIV. It can also raise the possibility of transmission through unsafe newborn feeding practices and worsening maternal health [ 32 ]. In addition, food insecurity has been linked to decreased antiretroviral adherence, declines in physical health status, worse immunologic status [ 33 ], decreased viral suppression [ 34 , 35 ], increased incidence of serious illness [ 36 ], and increased mortality [ 37 ] among people living with HIV.
With the above theoretical relationship between target variables and since this study focuses on the impact of food insecurity on health outcomes, and not on the causes, it adopted the conceptual framework of Weiser et al. [ 18 ] and constructed Fig. 1 .

A conceptual framework of food insecurity and health. Source: Modified and constructed by the author using Weiser et al. [ 18 ] conceptual framework. Permission was granted by Taylor & Francis to use their original Figs. (2.2, 2.3, and 2.4); to develop the above figure. Permission number: 1072954
Several findings associate food insecurity with poorer health, worse disease management, and a higher risk of premature mortality even though they used microdata. For instance, Stuff et al. [ 38 ] found that food insecurity is related to poor self-reported health status, obesity [ 39 ], abnormal blood lipids [ 40 ], a rise in diabetes [ 24 , 40 ], increased gestational diabetes[ 41 ], increased perceived stress, depression and anxiety among women [ 25 , 42 ], Human Immunodeficiency Virus (HIV) acquisition risk [ 43 , 44 , 45 ], childhood stunting [ 46 ], poor health [ 47 ], mental health and behavioral problem [ 25 , 48 , 49 ].
The above highlight micro-level empirical studies, and since the scope of this study is macro-level, Table 1 provides only the existing macro-level empirical findings related to the current study.
Empirical findings in Table 1 are a few, implying a limited number of macro-level level empirical findings. Even the existing macro-level studies have several limitations. For instance, most studies either employed conventional estimation techniques or overlooked basic econometric tests; thus, their results and policy implications may mislead policy implementers. Except for Hameed et al. [ 53 ], most studies’ data are either outdated or unbalanced; hence, their results and policy implications may not be valuable in the dynamic world and may not be accurate like balanced data. Besides, some studies used limited (one) sampled countries; however, few sampled countries and observations do not get the asymptotic properties of an estimator [ 56 ]. Therefore, this study tries to fill the existing gaps by employing robust estimation techniques with initial diagnostic and post-estimation tests, basic panel econometric tests and robustness checks, updated data, a large number of samples.
Study setting and participants
According to Smith and Meade [ 57 ], the highest rates of both food insecurity and severe food insecurity were found in Sub-Saharan Africa in 2017 (55 and 28%, respectively), followed by Latin America and the Caribbean (32 and 12%, respectively) and South Asia (30 and 13%). Similarly, SSA countries have worst health outcomes compared to other regions. For instance, in 2020, the region had the lowest life expectancy [ 58 ] and highest infant mortality [ 59 ]. Having the above information, this study's target population are SSA countries chosen purposively. However, even though SSA comprises 49 of Africa's 55 countries that are entirely or partially south of the Sahara Desert. This study is conducted for a sample of 31 SSA countries (Angola, Benin, Botswana, Burkina Faso, Cameroon, Cabo Verde, Chad, Congo Rep., Côte d'Ivoire, Ethiopia, Gabon, The Gambia, Ghana, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritania, Mauritius, Mozambique, Namibia, Nigeria, Rwanda, Senegal, Sierra Leone, South Africa, Sudan, Tanzania, and Togo). The sampled countries are selected based on data accessibility for each variable included in the empirical models from 2001 to 2018. Since SSA countries suffer from food insecurity and related health problems, this study believes the sampled countries are appropriate and represent the region. Moreover, since this study included a large sample size, it improves the estimator’s precision.
Data type, sources, and scope
This study uses secondary data collected in December 2020 online from the databases of the Food and Agricultural Organization (FAO), the United Nations Development Programme (UNDP), and the World Bank (WB) (see Table 2 ). In addition, the study uses yearly balanced data from 2001 to 2018, which is appropriate because it captures the Millennium Development Goals, SDGs, and other economic conditions, such as the rise of SSA countries’ economies and the global financial crisis of the 2000s. Therefore, this study considers various global development programs and events. Generally, the scope of this study (sampled countries and time) is sufficient to represent SSA countries. In other words, the study has n*T = 558 observations, which fulfills the large sample size criteria recommended by Kennedy [ 56 ].
The empirical model
Model specification is vital to conduct basic panel data econometric tests and estimate the relationship of target variables. Besides social factors, the study includes economic factors determining people's health status. Moreover, it uses two proxies indicators to measure both food insecurity and health status; hence, it specifies the general model as follows:
The study uses four models to analyze the impact of food insecurity on health outcomes.
where LNLEXP and LNINFMOR (dependent variables) refer to the natural logarithm of life expectancy at birth and infant mortality used as proxy variables for health outcomes. Similarly, PRUND and AVRDES are the prevalence of undernourishment and average dietary energy supply adequacy – proxy and predictor variables for food insecurity.
Moreover, to regulate countries’ socio-economic conditions and to account for time-varying bias that can contribute to changes in the dependent variable, the study included control variables, such as GDPPC, GOVEXP, MNSCHOOL, and URBAN. GDPPC is GDP per capita, GOVEXP refers to domestic general government health expenditure, MNSCHOOL is mean years of schooling and URBAN refers to urbanization. Further, n it , v it , ε it , and μ it are the stochastic error terms at period t. The parameters \({\alpha }_{0}, { \beta }_{0}, { \theta }_{0},{ \delta }_{0}\) refer to intercept terms and \({\alpha }_{1}-{\alpha }_{5}, {\beta }_{1}-{\beta }_{5}, { \theta }_{1}-{\theta }_{5}, and {\delta }_{1}-{\delta }_{5}\) are the long-run estimation coefficients. Since health outcomes and food insecurity have two indicators used as proxy variables, this study estimates different alternative models and robustness checks of the main results. Furthermore, the above models did not address heterogeneity problems; hence, this study considers unobserved heterogeneity by introducing cross-section and time heterogeneity in the models. This is accomplished by assuming a two-way error component for the disturbances with:
From Eq. 2 , the unobservable individual (cross-section) and unobservable time heterogeneities are described by \({\delta }_{i} and {\tau }_{t}\) (within components), respectively. Nonetheless, the remaining random error term is \({\gamma }_{it}\) (panel or between components). Therefore, the error terms in model 1A-1D will be substituted by the right-hand side elements of Eq. 2 .
Depending on the presumptions of whether the error elements are fixed or random, the FE and RE models are the two kinds of models that will be evaluated. Equation ( 2 ) yields a two-way FE error component model, or just a FE model if the assumptions are that \({\delta }_{i} and {\tau }_{t}\) are fixed parameters to be estimated and that the random error component, \({\gamma }_{it}\) , is uniformly and independently distributed with zero mean and constant variance (homoscedasticity).
Equation ( 2 ), on the other hand, provides a two-way RE error component model or a RE model if we suppose \({\delta }_{i} and {\tau }_{t}\) are random, just like the random error term, or \({\delta }_{i},{\tau }_{t}, and {\gamma }_{it}\) are all uniformly and independently distributed with zero mean and constant variance, or they are all independent of each other and independent variables [ 60 ].
Rather than considering both error components, \({\delta }_{i}, and {\tau }_{t}\) , we can examine only one of them at a time (fixed or random), yielding a one-way error component model, FE or RE. The stochastic error term \({\varpi }_{it}\) in Eq. 2 will then be:
Statistical analysis
This study conducted descriptive statistics, correlation analysis, and initial diagnosis tests (cross-sectional and time-specific fixed effect, outliers and influential observations, multicollinearity, normality, heteroscedasticity, and serial correlation test). Moreover, it provides basic panel econometric tests and panel data estimation techniques. For consistency, statistical software (STATA) version 15 was used for all analyses.
Descriptive statistics and correlation analysis
Descriptive statistics is essential to know the behavior of the variables in the model. Therefore, it captures information, such as the mean, standard deviation, minimum, maximum, skewness, and kurtosis. Similarly, the study conducted Pearson correlation analysis to assess the degree of relationship between the variables.
Initial diagnosis
Cross-sectional and time-specific fixed effect.
One can anticipate differences arising over time or within the cross-sectional units, given that the panel data set comprises repeated observations over the same units gathered over many periods. Therefore, before estimation, this study considered unexplained heterogeneity in the models. One fundamental limitation of cross-section, panel, and time series data regression is that they do not account for country and time heterogeneity [ 60 ]. These unobserved differences across nations and over time are crucial in how the error term is represented and the model is evaluated. These unobserved heterogeneities, however, may be represented by including both country and time dummies in the regression. However, if the parameters exceed the number of observations, the estimate will fail [ 60 ]. However, in this study, the models can be estimated. If we include both country and time dummies, we may assume that the slope coefficients are constant, but the intercept varies across countries and time, yielding the two-way error components model. As a result, this study examines the null hypothesis that intercepts differ across nations and time in general.
Detecting outliers and influential observations
In regression analysis, outliers and influential observations may provide biased findings. Therefore, the Cooks D outlier and influential observation test was used in the study to handle outliers and influencing observations. To evaluate whether these outliers have a stronger impact on the model to be estimated, each observation in this test was reviewed and compared with Cook’s D statistic [ 61 ]. Cook distance evaluates the extent to which observation impacts the entire model or the projected values. Hence, this study tested the existence of outliers.
Normality, heteroscedasticity, multicollinearity, and serial correlation test
Before the final regression result, the data used for the variables were tested for normality, heteroscedasticity, multicollinearity, and serial correlation to examine the characteristics of the sample.
Regression models should be checked for nonnormal error terms because a lack of Gaussianity (normal distribution) can occasionally compromise the accuracy of estimation and testing techniques. Additionally, the validity of inference techniques, specification tests, and forecasting critically depends on the normalcy assumption [ 62 ]. Similarly, multicollinearity in error terms leads to a dataset being highly sensitive to a minor change, instability in the regression model, and skewed and unreliable results. Therefore, this study conducted the normality using Alejo et al. [ 62 ] proposed command and multicollinearity (using VIF) tests.
Most conventional panel data estimation methods rely on homoscedastic individual error variance and constant serial correlation. Since the error component is typically connected to the variance that is not constant during the observation and is serially linked across periods, these theoretical presumptions have lately reduced the applicability of various panel data models. Serial correlation and heteroskedasticity are two estimate issues frequently connected to cross-sectional and time series data, respectively. Similarly, panel data is not free from these issues because it includes cross-sections and time series, making the estimated parameters ineffective, and rendering conclusions drawn from the estimation incorrect [ 63 ]. Therefore, this study used the Wooldridge [ 63 ] test for serial correlation in linear panel models as well as the modified Wald test for heteroskedasticity.
Basic panel econometric tests
The basic panel data econometric tests are prerequisites for estimating the panel data. The three main basic panel data tests are cross-sectional dependence, unit root, and cointegration.
Cross-sectional dependence (CD)
A growing body of the panel data literature concludes that panel data models are likely to exhibit substantial CD in the errors resulting from frequent shocks, unobserved components, spatial dependence, and idiosyncratic pairwise dependence. Even though the impact of CD in estimation depends on several factors, relative to the static model, the effect of CD in dynamic panel estimators is more severe [ 64 ]. Moreover, Pesaran [ 65 ] notes that recessions and economic or financial crises potentially affect all countries, even though they might start from just one or two countries. These occurrences inevitably introduce cross-sectional interdependencies across the cross-sectional unit, their regressors, and the error terms. Hence, overlooking the CD in panel data leads to biased estimates and spurious results [ 64 , 66 ]. Further, the CD test determines the type of panel unit root and cointegration tests we should apply. Therefore, examining the CD is vital in panel data econometrics.
In the literature, there are several tests for CD, such as the Breusch and Pagan [ 67 ] Lagrange multiplier (LM) test, Pesaran [ 68 ] scaled LM test, Pesaran [ 68 ] CD test, and Baltagi et al. [ 69 ] bias-corrected scaled LM test (for more detail, see Tugcu and Tiwari [ 70 ]). Besides, Friedman [ 71 ] and Frees [ 72 , 73 ] also have other types of CD tests (for more detail, see De Hoyos and Sarafidis [ 64 ]). This study employs Frees [ 72 ] and Pesaran [ 68 ] among the existing CD tests. This is because, unlike the Breusch and Pagan [ 67 ] test, these tests do not require infinite T and fixed N, and are rather applicable for both a large N and T. Additionally, Free’s CD test can overcome the irregular signs associated with correlation. However, it also employs Friedman [ 71 ] CD for mixed results of the above tests.
Unit root test
The panel unit root and cointegration tests are common steps following the CD test. Generally, there are two types of panel unit root tests: (1) the first-generation panel unit root tests, such as Im et al. [ 74 ], Maddala and Wu [ 75 ], Choi [ 76 ], Levin et al. [ 77 ], Breitung [ 78 ] and Hadri [ 79 ], and (2) the second-generation panel unit root tests, such as [ 66 , 80 , 81 , 82 , 83 , 84 , 85 , 86 , 87 , 88 , 89 ].
The first-generation panel unit root tests have been criticized because they assume cross-sectional independence [ 90 , 91 , 92 , 93 ]. This hypothesis is somewhat restrictive and unrealistic, as macroeconomic time series exhibit significant cross-sectional correlation among countries in a panel [ 92 ], and co-movements of economies are often observed in the majority of macroeconomic applications of unit root tests [ 91 ]. The cross-sectional correlation of errors in panel data applications in economics is likely to be the rule rather than the exception [ 93 ]. Moreover, applying first-generation unit root tests under CD models can generate substantial size distortions [ 90 ], resulting in the null hypothesis of nonstationary being quickly rejected [ 66 , 94 ]. As a result, second-generation panel unit root tests have been proposed to take CD into account. Therefore, among the existing second-generation tests, this study employs Pesaran’s [ 66 ] cross-sectionally augmented panel unit root test (CIPS) for models 1A–1C . The rationale for this is that, unlike other unit root tests that allow CD, such as Bai and Ng [ 80 ], Moon and Perron [ 87 ], and Phillips and Sul [ 84 ], Pesaran’s [ 66 ] test is simple and clear. Besides, Pesaran [ 66 ] is robust when time-series’ heteroscedasticity is observed in the unobserved common factor [ 95 ]. Even though theoretically, Moon and Perron [ 87 ], Choi [ 96 ] and Pesaran [ 66 ] require large N and T, Pesaran [ 66 ] is uniquely robust in small sample sizes [ 97 ]. Therefore, this study employs the CIPS test to take into account CD, and heteroskedasticity in the unobserved common factor and both large and small sample countries. However, since there is no CD in model 1D , this study employs the first-generation unit root tests called Levin, Lin, and Chu (LLC), Im, Pesaran, Shin (IPS) and Fisher augmented Dickey–Fuller (ADF) for model 1D .
Cointegration test
The most common panel cointegration tests when there is CD are Westerlund [ 98 ], Westerlund and Edgerton [ 99 ], Westerlund and Edgerton [ 100 ], Groen and Kleibergen [ 101 ], Westerlund’s [ 102 ] Durbin-Hausman test, Gengenbach et al. [ 103 ] and Banerjee and Carrion-i-Silvestre [ 104 ]. However, except for a few, most tests are not coded in Statistical Software (STATA) and are affected by insufficient observations. The current study primarily uses Westerlund [ 98 ] and Banerjee and Carrion-i-Silvestre [ 104 ] for models 1A–1C . However, to decide uncertain results, it also uses McCoskey and Kao [ 105 ] cointegration tests for model 1C . The rationale for using Westerlund’s [ 98 ] cointegration test is that most panel cointegration has failed to reject the null hypothesis of no cointegration due to the failure of common-factor restriction [ 106 ]. However, Westerlund [ 98 ] does not require any common factor restriction [ 107 ] and allows for a large degree of heterogeneity (e.g., individual-specific short-run dynamics, intercepts, linear trends, and slope parameters) [ 92 , 107 , 108 ]. Besides, its command is coded and readily available in STATA. However, it suffers from insufficient observations, especially when the number of independent variables increases. The present study employs the Banerjee and Carrion-i-Silvestre [ 104 ] and McCoskey and Kao [ 105 ] cointegration tests to overcome this limitation. The two Engle-Granger-based cointegration tests applicable when there is no CD and are widely used and available in STATA are Pedroni [ 109 , 110 ] and Kao [ 111 ]. However, the Pedroni test has two benefits over Kao: it assumes cross-sectional dependency and considers heterogeneity by employing specific parameters [ 112 ]. Hence, this study uses the Pedroni cointegration test for model 1D .
Panel data estimation techniques
The panel data analysis can be conducted using different estimation techniques and is mainly determined by the results of basic panel econometric tests. Thus, this study mainly employs the Driscoll-Kraay [ 113 ] standard error (DKSE) (for models 1A and 1B ), FE (for model 1C ), and two-step GMM (for model 1D ) estimation techniques to examine the impact of food insecurity on health outcomes. It also employs the Granger causality test. However, for robustness checks, it uses fully modified ordinary least squares (FMOLS), panel-corrected standard error (PCSE), and feasible generalized least squares (FGLS) methods (for models 1A and 1B ). Moreover, it uses a random effect (RE) for model 1C and panel dynamic fixed effect (DFE) techniques for model 1D .
Even though several panel estimation techniques allow CD, most of them – such as cross-section augmented autoregressive distributed lag (CS-ARDL), cross-section augmented distributed lag (CS-DL), common correlated effects pooled (CCEP), and common correlated effects mean group (CCEMG) estimators – require a large number of observations over groups and periods. Similarly, the continuously updated fully modified (CUP-FM) and continuously updated bias-corrected (CUP-BC) estimators are not coded in STATA. Others, like the PCSE, FGLS, and seemingly unrelated regression (SUR), are feasible for T (the number of time series) > N (the number of cross-sectional units) [ 114 , 115 ]. However, a DKSE estimate is feasible for N > T [ 114 ]. Therefore, depending on the CD, cointegration test, availability in STATA, and comparing N against T, this study mainly employs the DKSE regression for models 1A and 1B , FE model for model 1C , and GMM for model 1C .
Finally, to check the robustness of the main result, this study employs FMOLS, FGLS, and PCSE estimation techniques for models 1A and 1B . Furthermore, even though the Hausman test confirms that the FE is more efficient, the study employs the RE for model 1C . This is because Firebaugh et al. [ 116 ] note that the RE and FE models perform best in panel data. Besides, unlike FE, RE assumes that individual differences are random. In addition, this study uses panel DFE for model 1D (selected based on the Hausman test). Finally, the robustness check is also conducted using an alternative model (i.e., when a dependent variable is without a natural log and Granger causality test).
Table 3 shows the overall mean of LNLEXP of the region is 4.063 years which indicates that the region can achieve only 57.43 (using ln(x) = 4.063 = loge (x) = e 4.063 , where e = 2.718) years of life expectancy. This is very low compared to other regions. Besides, the ranges in the value of LNLEXP are between 3.698 and 4.345 or (40–76 years), implying high variation. Similarly, the mean value of LNINFMOR is 3.969; implying SSA countries recorded 52 infants death per 1000. Moreover, the range of LNINFMOR is between 2.525 and 4.919 or (12 – 135 infant death per 1000), implying high variation within the region. The mean value of people’s prevalence for undernourishment is 21.26; indicating 21% of the population is undernourished. However, the mean value of AVRDES is 107.826, which is greater than 100, implying that the calorie supply is adequate for all consumers if the food is distributed according to the requirements of individuals. When we observe the skewness and kurtosis of the variables of the models, except for LNLEXP and LNINFMOR, all variables are positively skewed. In addition, all variables have positive kurtosis with values between 2.202 and 6.092.
Table 3 also shows the degree of relationship between variables, such that most values are below the threshold or rule of thumb (0.7) for a greater association [ 117 ]. However, the association between LNINFMOR and LNLEXP, as well as between PRUNP and AVRDES, is over the threshold and seems to have a multicollinearity issue. Nevertheless, these variables did not exist together in the models, indicating the absence of a multicollinearity problem.
Table 4 shows whether the cross-sectional specific and time-specific FE in extended models ( model 1A-1D plus Eq. 2 ) are valid. The result reveals that the null hypothesis of the captured unobserved heterogeneity is homogenous across the countries, and time is rejected at 1%, implying the extended models are correctly specified. Besides, to check the robustness of the two-way error component model relative to the pooled OLS estimator, this study conducted an additional poolability test. The result shows the null hypothesis that intercepts homogeneity (pooling) is rejected at a 1% level; thus, the FE model is most applicable, but the pooled OLS is biased.
Cooks D is an indicator of high leverage and residuals. The impact is high when D exceeds 4/N, (N = number of observations). A D > 1 implies a significant outlier problem. The Cooks D result of this study confirms the absence of outliers' problem (see supplementary file 1 ).
Normality, heteroscedasticity, serial correlation, and multicollinearity tests
The results in Table 5 indicate that the probability value of the joint test for normality on e and u are above 0.01, implying that the residuals are normally distributed. The heteroscedasticity results show that the probability value of the chi-square statistic is less than 0.01 in all models. Therefore, the null hypothesis of constant variance can be rejected at a 1% level of significance. In other words, the modified Wald test result for Groupwise heteroskedasticity presented in Table 5 , rejects the null hypothesis of Groupwise homoskedasticity observed by the probability value of 0.0000, which implies the presence of heteroscedasticity in the residuals. Similarly, all models suffer from serial correlation since the probability value of 0.0000 rejects the null hypothesis of no first-order serial correlation, indicating the presence of autocorrelation in all panel models. Finally, the multicollinearity test reveals that the models have no multicollinearity problem since the Variance inflation Factors (VIF) values are below 5.
Cross-sectional dependence test
Results in Table 6 strongly reject the null hypothesis of cross-sectional independence for models 1A – 1C . However, for model 1D , the study found mixed results (i.e., Pesaran [ 68 ] fails to reject the null hypothesis of no CD while Frees [ 72 ] strongly rejects it). Thus, to decide, this study employs the Friedman [ 71 ] CD test. The result fails to reject the null hypothesis of cross-sectional independence, implying that two out of three tests fail to reject the null hypothesis of cross-sectional independence in model 1D . Therefore, unlike others, there is no CD in model 1D (see Table 6 ).
Unit root tests
Table 7 shows that all variables are highly (at 1% level) significant either at level (I(0)) or first difference (I(1)), which implies all variables are stationary. In other words, the result fails to reject the null hypothesis of unit root (non-stationary) for all variables at a 1%-significance level, either at levels or the first differences. Thus, we might expect a long-run connection between these variables collectively.
Cointegration tests
The results in Table 8 show that both the Westerlund [ 98 ] and Banerjee and Carrion-i-Silvestre [ 104 ] cointegration tests strongly reject the null hypothesis of no-cointegration in models 1A and 1B . However, model 1C provides a mixed result, i.e. the Banerjee and Carrion-i-Silvestre [ 104 ] test rejects the null hypothesis of no cointegration, yet the reverse is true for the Westerlund [ 98 ] test. Therefore, this study conducted further cointegration tests for model 1C . Even though Westerlund and Edgerton [ 99 ] suffer from insufficient observation, it is based on the McCoskey and Kao [ 105 ] LM test [ 118 ]. Thus, we can use a residual-based cointegration test in the heterogeneous panel framework proposed by McCoskey and Kao [ 105 ]. However, an efficient estimation technique of cointegrated variables is required, and hence the FMOLS and DOLS estimators are recommended. The residuals derived from the FMOLS and DOLS will be tested for stationarity with the null hypothesis of no cointegration amongst the regressors. Since the McCoskey and Kao [ 105 ] test involves averaging the individual LM statistics across the cross-sections, for testing the residuals FMOLS and DOLS stationarity, McCoskey, and Kao [ 105 ] test is in the spirit of IPS (Im et al. [ 74 ]) [ 119 ].
Though FMOLS and DOLS are recommended for the residuals cointegration test, DOLS is better than FMOLS (for more detail, see Kao and Chiang [ 120 ]); therefore, this study uses a residual test derived from DOLS. The result fails to reject the null hypothesis of no cointegration. Two (Banerjee and Carrion-i-Silvestre [ 104 ] and McCoskey and Kao [ 105 ]) out of three tests fail to reject the null hypothesis of no cointegration; hence, we can conclude that there is no long-run relationship among the variables in model 1C .
Unlike other models, since there is CD in model 1D , this study employs the Pedroni [ 109 ] and Kao [ 111 ] cointegration tests for model 1D . The result strongly rejects the null hypothesis of no cointegration, which is similar to models 1A and 1B , that a long-run relationship exists among the variables in model 1D (see Table 5 ).
Panel data estimation results
Table 9 provides long-run regression results of all models employing appropriate estimation techniques such as DKSE, FE, and two-step GMM, along with the Granger causality test. However, the DKSE regression can be estimated in three ways: FE with DKSE, RE with DKSE, and pooled Ordinary Least Squares/Weighted Least Squares (pooled OLS/WLS) regression with DKSE. Hence, we must choose the most efficient model using Hausman and Breusch-Pagan LM for RE tests (see supplementary file 2 ). As a result, this study employed FE with DKSE for models 1A and 1B . Further, due to Hausman's result, absence of cointegration and to deal with heterogeneity and spatial dependence in the dynamic panel, this study employs FE for the model1C (see the supplementary file 2). However, due to the absence of CD, the presence of cointegration, and N > T, this study uses GMM for model 1D . Moreover, according to Roodman [ 121 ], the GMM approach can solve heteroskedasticity and autocorrelation problems. Furthermore, even though two-step GMM produces only short-run results, it is possible to generate long-run coefficients from short-run results [ 122 , 123 ].
The DKSE result of model 1A shows that a 1% increment in people's prevalence for undernourishment reduces their life expectancy by 0.00348 PPs (1 year or 366 days). However, in model 1C, a 1% rise in the prevalence of undernourishment increases infant mortality by 0.0119 PPs (1 year or 369 days). The DKSE estimations in model 1B reveal that people’s life expectancy rises by 0.00317 PPs with every 1% increase in average dietary energy supply. However, the GMM result for model 1D confirms that a 1% incrementin average dietary energy supply reduces infant mortality by 0.0139 PPs. Moreover, this study conducted a panel Granger causality test to confirm whether or not food insecurity has a potential causality to health outcomes. The result demonstrates that the null hypothesis of change in people’s prevalence for undernourishment and average dietary energy supply does not homogeneously cause health outcomes is rejected at 1% significance, implying a change in food insecurity does Granger-cause health outcomes of SSA countries (see Table 9 ).
In addition to the main results, Table 9 also reports some post-estimation statistics to ascertain the consistency of the estimated results. Hence, in the case of DKSE and FE models, the validity of the models is determined by the values of R 2 and the F statistics. For instance, R 2 quantifies the proportion of the variance in the dependent variable explained by the independent variables, representing the model’s quality. The results in Table 9 demonstrate that the explanatory variables explain more than 62% of the variance on the dependent variable. Cohen [ 125 ] classifies the R 2 value of 2% as a moderate influence in social and behavioral sciences, while 13 and 26% are considered medium and large effects, respectively. Therefore, the explanatory variables substantially impact this study's models. Similarly, the F statistics explain all independent variables jointly explain the dependent one. For the two-step system GMM, the result fails to reject the null hypothesis of no first (AR(1)) and second-order (AR(2)) serial correlation, indicating that there is no first and second-order serial correlation. In addition, the Hansen [ 126 ] and Sargan [ 127 ] tests fail to reject the null hypothesis of the overall validity of the instruments used, which implies too many instruments do not weaken the model.
Robustness checks
The author believes the above findings may not be enough for policy recommendations unless robustness checks are undertaken. Hence, the study estimated all models without the natural logarithm of the dependent variables (see Table 10 ). The model 1A result reveals, similar to the above results, individuals’ prevalence for undernourishment significantly reduces their life expectancy in SSA countries. That means a 1% increase in the people's prevalence of undernourishment reduces their life expectancy by 0.1924 PPs. Moreover, in model 1B , life expectancy rises by 0.1763 PPs with every 1% increase in average dietary energy supply. In model 1C , the rise in infants’ prevalence for undernourishment has a positive and significant effect on their mortality rate in SSA countries. The FE result implies that a 1% rise in infants’ prevalence for undernourishment increases their mortality rate by 0.9785 PPs. The GMM result in model 1D indicates that improvement in average dietary energy supply significantly reduces infant mortality. Further, the Granger causality result confirms that the null hypothesis of change in the prevalence of undernourishment and average dietary energy supply does not homogeneously cause health outcomes and is rejected at a 1% level of significance. This implies a change in food insecurity does Granger-cause health outcomes in SSA countries (see Table 10 ).
The study also conducted further robustness checks using the same dependent variables (as Table 9 ) but different estimation techniques. The results confirm that people’s prevalence of undernourishment has a negative and significant effect on their life expectancy, but improvement in average dietary energy supply significantly increases life expectancy in SSA countries. However, the incidence of undernourishment in infants contributes to their mortality; however, progress in average dietary energy supply for infants significantly reduces their mortality (see Table 11 ).
The main objective of this study is to examine the impact of food insecurity on the health outcomes of SSA countries. Accordingly, the DKSE result of model 1A confirms that the rise in people’s prevalence for undernourishment significantly reduces their life expectancy in SSA countries. However, the FE result shows that an increment in the prevalence of undernourishment has a positive and significant impact on infant mortality in model 1C . This indicates that the percentage of the population whose food intake is insufficient to meet dietary energy requirements is high, which leads to reduce life expectancy but increases infant mortality in SSA countries. The reason for this result is linked to the insufficient food supply in SSA due to low production and yields, primitive tools, lack of supporting smallholder farms and investment in infrastructure, and government policies. Besides, even though the food is available, it is not distributed fairly according to the requirements of individuals. Moreover, inadequate access to food, poor nutrition, and chronic illnesses are caused by a lack of well-balanced diets. In addition, many of these countries are impacted by poverty, making it difficult for citizens to afford nutritious food. All these issues combine to create an environment where individuals are more likely to suffer malnutrition-related illnesses, resulting in a lower life expectancy rate. The DKSE estimation result in model 1B reveals that improvement in average dietary energy supply positively impacts people's life expectancy in SSA countries. However, the improvement in average dietary energy supply reduces infant mortality.
Based on the above results, we can conclude that food insecurity harms SSA nations' health outcomes. This is because the prevalence of undernourishment leads to increased infant mortality by reducing the vulnerability, severity, and duration of infectious diseases such as diarrhea, pneumonia, malaria, and measles. Similarly, the prevalence of undernourishment can reduce life expectancy by increasing the vulnerability, severity, and duration of infectious diseases. However, food security improves health outcomes – the rise in average dietary energy supply reduces infant mortality and increases the life expectancy of individuals.
Several facts and theories support the above findings. For instance, similar to the theoretical and conceptual framework section, food insecurity in SSA countries can affect health outcomes in nutritional, mental health, and behavioral channels. According to FAO et al. [ 128 ], the prevalence of undernourishment increased in Africa from 17.6% of the population in 2014 to 19.1% in 2019. This figure is more than twice the global average and the highest of all regions of the world. Similarly, SSA is the world region most at risk of food insecurity [ 129 ]. According to Global Nutrition [ 130 ] report, anemia affects an estimated 39.325% of women of reproductive age. Some 13.825% of infants have a low weight at birth in the SSA region. Excluding middle African countries (due to lack of data), the estimated average prevalence of infants aged 0 to 5 months who are exclusively breastfed is 35.73%, which is lower than the global average of 44.0%. Moreover, SSA Africa still experiences a malnutrition burden among children aged under five years. The average prevalence of overweight is 8.15%, which is higher than the global average of 5.7%. The prevalence of stunting is 30.825%—higher than the worldwide average of 22%. Conversely, the SSA countries’ prevalence of wasting is 5.375%, which is higher than most regions such as Central Asia, Eastern Asia, Western Asia, Latin America and the Caribbean, and North America. The SSA region's adult population also faces a malnutrition burden: an average of 9.375% of adult (aged 18 and over) women live with diabetes, compared to 8.25% of men. Meanwhile, 20.675% of women and 7.85% of men live with obesity.
According to Saltzman et al. [ 17 ], micronutrient deficiencies can affect people’s health throughout their life cycle. For instance, at the baby age, it causes (low birth weight, higher mortality rate, and impaired mental development), child (stunting, reduced mental capacity, frequent infections, reduced learning capacity, higher mortality rate), adolescent (stunting, reduced mental capacity, fatigue, and increased vulnerability to infection), pregnant women (increased mortality and perinatal complications), adult (reduced productivity, poor socio-economic status, malnutrition, and increased risk of chronic disease), elderly (increased morbidity (including osteoporosis and mental impairment), and higher mortality rate).
Though this study attempts to fill the existing gaps, it also has limitations. It examined the impact of food insecurity on infant mortality; however, their association is reflected indirectly through other health outcomes. Hence, future studies can extend this study by examining the indirect effect of food insecurity on infant mortality, which helps to look at in-depth relationships between the variables. Moreover, this study employed infant mortality whose age is below one year; hence, future studies can broaden the scope by decomposing infant mortality into (neonatal and postnatal) and under-five mortality.
Millions of people are dying every year due to hunger and hunger-related diseases worldwide, especially in SSA countries. Currently, the link between food insecurity and health status is on researchers' and policymakers' agendas. However, macro-level findings in this area for most concerned countries like SSA have been given only limited attention. Therefore, this study examined the impact of food insecurity on life expectancy and infant mortality rates. The study mainly employs DKSE, FE, two-step GMM, and Granger causality approaches, along with other estimation techniques for robustness checks for the years between 2001 and 2018. The result confirms that food insecurity harms health outcomes, while food security improves the health status of SSA nations'. That means that a rise in undernourishment increases the infant mortality rate and reduces life expectancy. However, an improvement in the average dietary energy supply reduces infant mortality and increases life expectancy. Therefore, SSA countries need to guarantee their food accessibility both in quality and quantity, which improves health status. Both development experts and political leaders agree that Africa has the potential for agricultural outputs, can feed the continent, and improve socio-economic growth. Besides, more than half of the world's unused arable land is found in Africa. Therefore, effective utilization of natural resources is essential to achieve food security. Moreover, since the majority of the food in SSA is produced by smallholder farmers [ 131 ] while they are the most vulnerable to food insecurity and poverty [ 132 , 133 ]; hence, special focus and support should be given to smallholder farmers that enhance food self-sufficiency. Further, improvement in investment in agricultural research; improvement in markets, infrastructures, and institutions; good macroeconomic policies and political stability; and developing sub-regional strategies based on their agroecological zone are crucial to overcoming food insecurity and improving health status. Finally, filling a stomach is not sufficient; hence, a person's diet needs to be comprehensive and secure, balanced (including all necessary nutrients), and available and accessible. Therefore, SSA countries should ensure availability, accessibility, usability, and sustainability to achieve food and nutrition security.
Availability of data and materials
The datasets used and/or analyzed during the current study are available in supplementary materials.
Abbreviations
Augmented Dickey–Fuller
Acquired Immunodeficiency Syndrome
Average Dietary Energy Supply
Common Correlated Effects Mean Group
Common Correlated Effects Pooled
Cross-Sectional Dependence
Cross-Sectionally Augmented Panel Unit Root Test
Cross-Section Augmented Autoregressive Distributed Lag
Cross-Section Augmented Distributed Lag
Continuously Updated Bias-Corrected
Continuously Updated Full Modified
Dynamic Fixed Effect
Driscoll-Kraay Standard Errors
Dynamic Ordinary Least Square
Error Correction Model
Food and Agricultural Organization
Fixed Effect
Feasible Generalised Least Squares
Fully Modified Ordinary Least Square
Gross Domestic Product (GDP) per capita
Generalised Method of Momentum
Domestic General Government Health Expenditure
Human Immunodeficiency Virus
Integration at First Difference
International Fund for Agricultural Development
Infant Mortality Rate
Im, Pesaran, Shin
Lag of Infant Mortality Rate
Lag of Natural Logarithm of Infant Mortality Rate
Life Expectancy at Birth
Levin, Lin, and Chu
Lagrange Multiplier
Natural Logarithm of Infant Mortality Rate
Natural Logarithm of Life Expectancy at Birth
Mean Years of Schooling
Ordinary Least Squares
Panel-Corrected Standard Error
Pooled Mean Group
Prevalence of Undernourishment
Random Effect
Sustainable Development Goals
Sub-Saharan African
Statistical Software
Seemingly Unrelated Regression
Urbanisation
World Food Programme
World Health Organization
Weighted Least Squares
Giller KE. The food security conundrum of sub-Saharan Africa. Glob Food Sec. 2020;2020(26): 100431.
Article Google Scholar
WHO. Reducing risks, promoting healthy life. World Health Report. Switzerland: WHO; 2002. Available from: https://apps.who.int/iris/bitstream/handle/10665/42510/WHR_2002.pdf?sequence=1 .
Food Research and Action Center. Hunger and health: the impact of poverty, food insecurity, and poor nutrition on health and well-being. Washington, DC: Food Research & Action Center; 2017. https://frac.org/research/resource-library/hunger-health-impact-poverty-food-insecurity-poor-nutrition-health-well .
Google Scholar
FAO, IFAD, WFP. The State of Food Insecurity in the World 2013. The multiple dimensions of food security. Rome: Food and Agriculture Organization of the United Nations; 2013. Available from: http://www.fao.org/3/i3434e/i3434e00.htm .
Roser M, Ritchie H. Hunger, and Undernourishment. Oxford: University of Oxford; 2013. Available from: https://ourworldindata.org/hunger-and-undernourishment .
Word Count. How many people die from hunger each year. Denmark: The World Counts; 2020. Available from: https://www.theworldcounts.com/challenges/people-and-poverty/hunger-and-obesity/how-many-people-die-from-hunger-each-year/story .
FAO IFAD, UNICEF, WFP, and WHO. The State of Food Security and Nutrition in the World 2018. Building Climate Resilience for Food Security and Nutrition. Technical report. FAO. 11 September 2018. Available from: https://www.fao.org/3/I9553EN/i9553en.pdf or https://www.wfp.org/publications/2018-state-food-security-and-nutrition-world-sofi-report .
FAO, ECA, AUC. Africa regional overview of food security and nutrition 2019 -in brief. 2020.
UNHCR. UNHCR describes the alarming health and nutrition situation in South Sudan camps. News Stories, 24 August 2012. Available from: http://www.unhcr.org/503881659.html .
Laxmaiah A, Arlappa N, Balakrishna N, Mallikarjuna RK, Galreddy C, Kumar S, Ravindranath M, Brahmam GN. Prevalence and determinants of micronutrient deficiencies among rural children of eight states in India. Ann NutrMetab. 2013;62(3):231–41.
CAS Google Scholar
Muthayya S, Rah JH, Sugimoto JD, Roos FF, Kraemer K, Black RE. The global hidden hunger indices and maps: an advocacy tool for action. PLoS ONE. 2013;8(6): e67860.
Article CAS PubMed PubMed Central Google Scholar
SOS. Hunger and Food Scarceness in Africa. Washington, DC: SOS Children’s Villages; 2018. Available from: https://www.sos-usa.org/about-us/where-we-work/africa/hunger-in-africa .
Gulliford MC, Mahabir D, Rocke B. Food insecurity, food choices, and body mass index in adults: nutrition transition in Trinidad and Tobago. Int J Epidemiol. 2003;32:508–16.
Article PubMed Google Scholar
Stuff JE, Casey PH, Szeto K, Gossett J, Weber J, Simpson P, et al. Household food insecurity and adult chronic disease in the lower Mississippi delta. J Federation Am Soc Experiment Biol. 2005;19:A986.
Parker ED, Widome R, Nettleton JA, Pereira MA. Food security and metabolic syndrome in U.S. adults and adolescents: findings from the National Health and Nutrition Examination Survey 1999-2006. Ann Epidemiol. 2010;20:364–70.
Article PubMed PubMed Central Google Scholar
WHO. Global Prevalence of Vitamin A Deficiency in Populations at Risk 1995–2005: WHO Global Database on Vitamin A Deficiency. 2009. Available from: www.who.int/vmnis/vitamina/en/ .
Saltzman A, Birol E, Wiesman D, Prasai N, Yohannes Y, Menon P, Thompson J. 2014 global hunger index: The challenge of hidden hunger. Washington, DC: International Food Policy Research Institute; 2014.
Weiser SD, Palar K, Hatcher AM, Young SL, Frongillo EA. Food insecurity and health: a conceptual framework. In: Ivers L, editors. Food insecurity and public health (pp. 23-50). 1st ed. Boca Raton: CRC Press; 2015.
Rose D. Economic determinants and dietary consequences of food insecurity in the United States. J Nutr. 1999;129(2):517S-S520.
Article CAS PubMed Google Scholar
Dixon LB, Winkleby MA, Radimer KL. Dietary intakes and serum nutrients differ between adults from food-insufficient and food-sufficient families: Third National Health and Nutrition Examination Survey, 1988–1994. J Nutr. 2001;131(4):1232–46.
Kirkpatrick SI, Tarasuk V. Food insecurity is associated with nutrient inadequacies among Canadian adults and adolescents. J Nutr. 2008;138(3):604–12.
Schaible UE, Kaufmann SH. Malnutrition and infection: complex mechanisms and global impacts. PLoS Med. 2007;4(5): e115.
Laraia B, Epel E, Siega-Riz AM. Food insecurity with the experience of restrained eating is a recipe for increased gestational weight gain. Appetite. 2013;65:178–84.
Seligman HK, Bindman AB, Vittinghoff E, Kanaya AM, Kushel MB. Food insecurity is associated with diabetes mellitus: results from the National Health Examination and Nutrition Examination Survey (NHANES) 1999–2002. J Gen Intern Med. 2007;22(7):1018–23.
Whitaker RC, Phillips SM, Orzol SM. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics. 2006;118(3):e859–68.
Black PH, Garbutt LD. Stress, inflammation, and cardiovascular disease. J Psychosom Res. 2002;52(1):1–23.
Cunningham WE, Andersen RM, Katz MH, Stein MD, Turner BJ, Crystal S, Zierler S, Kuromiya K, Morton SC, St. Clair P, Bozzette SA. The impact of competing subsistence needs and barriers on access to medical care for persons with human immunodeficiency virus receiving care in the United States. Med Care. 1999;37(12):1270–81.
Kushel MB, Gupta R, Gee L, Haas JS. Housing instability and food insecurity as barriers to health care among low-income Americans. J Gen Intern Med. 2006;21(1):71–7.
Weiser SD, Tuller DM, Frongillo EA, Senkungu J, Mukiibi N, Bangsberg DR. Food insecurity as a barrier to sustained antiretroviral therapy adherence in Uganda. PLoS ONE. 2010;5(4): e10340.
Bengle R, Sinnett S, Johnson T, Johnson MA, Brown A, Lee JS. Food insecurity is associated with cost-related medication non-adherence in community-dwelling, low-income older adults in Georgia. J Nutr Elder. 2010;29(2):170–91.
Weiser SD, Leiter K, Bangsberg DR, Butler LM, Percy-de Korte F, Hlanze Z, Phaladze N, Iacopino V, Heisler M. Food insufficiency is associated with high-risk sexual behavior among women in Botswana and Swaziland. PLoS med. 2007;4(10): e260.
Mehta S, Manji KP, Young AM, Brown ER, Chasela C, Taha TE, Read JS, Goldenberg RL, Fawzi WW. Nutritional indicators of adverse pregnancy outcomes and mother-to-child transmission of HIV among HIV-infected women. Am J ClinNutr. 2008;87(6):1639–49.
Weiser SD, Bangsberg DR, Kegeles S, Ragland K, Kushel MB, Frongillo EA. Food insecurity among homeless and marginally housed individuals living with HIV/AIDS in San Francisco. AIDS Behav. 2009;13(5):841–8.
Weiser SD, Frongillo EA, Ragland K, Hogg RS, Riley ED, Bangsberg DR. Food insecurity is associated with incomplete HIV RNA suppression among homeless and marginally housed HIV-infected individuals in San Francisco. J Gen Intern Med. 2009;24(1):14–20.
Kalichman SC, Cherry C, Amaral C, White D, Kalichman MO, Pope H, Swetsze C, Jones M, Macy R. Health and treatment implications of food insufficiency among people living with HIV/AIDS, Atlanta. Georgia J Urban Health. 2010;87(4):631–41.
Weiser SD, Gupta R, Tsai AC, Frongillo EA, Grede N, Kumbakumba E, Kawuma A, Hunt PW, Martin JN, Bangsberg DR. Changes in food insecurity, nutritional status, and physical health status after antiretroviral therapy initiation in rural Uganda. J Acquir Immune DeficSyndr (1999). 2012;61(2):179.
Article CAS Google Scholar
Weiser SD, Fernandes KA, Brandson EK, Lima VD, Anema A, Bangsberg DR, Montaner JS, Hogg RS. The association between food insecurity and mortality among HIV-infected individuals on HAART. J Acquir Immune DeficSyndr (1999). 2009;52(3):342.
Stuff JE, Casey PH, Szeto KL, Gossett JM, Robbins JM, Simpson PM, et al. Household food insecurity is associated with adult health status. J Nutr. 2004;134(9):2330–5.
Dinour LM, Bergen D, Yeh MC. The food insecurity–obesity paradox: a review of the literature and the role food stamps may play. J Am Diet Assoc. 2007;107(11):1952–61.
Seligman HK, Davis TC, Schillinger D, Wolf MS. Food insecurity is associated with hypoglycemia and poor diabetes self-management in a low-income sample with diabetes. J Health Care Poor U. 2010;21(4):1227.
Laraia B, Siega-Riz AM, Gundersen C. Household food insecurity is associated with self-reported pregravid weight status, gestational weight gain, and pregnancy complications. J Am Diet Assoc. 2010;110:692–701.
Laraia BA, Siega-Riz AM, Gundersen C, Dole N. Psychosocial factors and socioeconomic indicators are associated with household food insecurity among pregnant women. J Nutr. 2006;136:177–82.
Miller CL, Bangsberg DR, Tuller DM, Senkungu J, Kawuma A, Frongillo EA, et al. Food insecurity and sexual risk in an HIV endemic community in Uganda. AIDS Behav. 2011;15(7):1512–9.
Tsai AC, Bangsberg DR, Frongillo EA, Hunt PW, Muzoora C, Martin JN, et al. Food insecurity, depression and the modifying role of social support among people living with HIV/AIDS in rural Uganda. SocSci Med. 2012;74(12):2012–9.
Vogenthaler NS, Kushel MB, Hadley C, Frongillo EA, Riley ED, Bangsberg DR, et al. Food insecurity and risky sexual behaviors among homeless and marginally housed HIV-infected individuals in San Francisco. AIDS Behav. 2013;17(5):1688–93.
Baig-Ansari N, Rahbar MH, Bhutta ZA, Badruddin SH. Child’s Child’s gender and household food insecurity are associated with stunting among young Pakistani children residing in urban squatter settlements. Food Nutr Bull. 2006;27(2):114–27.
Gundersen C, Kreider B. Bounding the effects of food insecurity on children’s health outcomes. J Health Econ. 2009;28(5):971–83.
Cole SM, Tembo G. The effect of food insecurity on mental health: panel evidence from rural Zambia. SocSci Med. 2011;73(7):1071–9.
Weaver LJ, Owens C, Tessema F, Kebede A, Hadley C. Unpacking the “black box” of global food insecurity and mental health. SocSci Med. 2021;282: 114042.
Uchendu FN. Hunger influenced life expectancy in war-torn Sub-Saharan African countries. J Health PopulNutr. 2018;37(1):1–4.
Asiseh F, Naanwaab C, Quaicoe O. The association between food insecurity and child health outcomes in low and middle-income countries. J Afr Dev. 2018;20(2):79–90.
Justice AE, Louis AA. The nexus between food security and infant mortality-further evidence from Nigeria. Amity J Econ. 2018;3(1):1–5.
Hameed S, Wei W, Chaudhary N. A dynamics appraisal of association among food Insecurity, women and child health: Evidence from developing countries. 2020. Available from: https://www.preprints.org/manuscript/202007.0291/v1 .
Banerjee S, Radak T, Khubchandani J, Dunn P. Food insecurity and mortality in American adults: results from the NHANES-linked mortality study. Health PromotPract. 2021;22(2):204–14.
Cassidy-Vu L, Way V, Spangler J. The correlation between food insecurity and infant mortality in North Carolina. Public Health Nutr. 2022;25(4):1038–44.
Kennedy P. A guide to econometrics. 6th ed. Toronto: Wiley-Blackwell; 2008.
Smith MD, Meade B. Who Are the World’s Food Insecure? Identifying the Risk Factors of Food Insecurity around the World. Amber Waves: 2019. The Economics of Food, Farming, Natural Resources, and Rural America. Available from: https://www.ers.usda.gov/amber-waves/2019/june/who-are-the-world-s-food-insecure-identifying-the-risk-factors-of-food-insecurity-around-the-world/ .
The World Bank. Life expectancy at birth, total (years). 2022a. Available from: https://data.worldbank.org/indicator/SP.DYN.LE00.IN .
The World Bank. Mortality rate, infant (per 1,000 live births). 2022b. Available from: https://data.worldbank.org/indicator/SP.DYN.IMRT.IN
Vijayamohanan PN. Panel data analysis with Stata Part 1 fixed effects and random effects models. 2016. MPRA Paper. Available from: https://mpra.ub.uni-muenchen.de/76869/1/MPRA_paper_76869.pdf .
Cook RD. Detection of influential observation in linear regression. Technometrics. 1977;19:15–8.
Alejo J, Galvao A, Montes-Rojas G, Sosa-Escudero W. Tests for normality in linear panel-data models. Stand Genomic Sci. 2015;15(3):822–32.
Wooldridge JM. Econometric Analysis of Cross Section and Panel Data. 2nd ed. Cambridge, MA: MIT Press; 2010.
De Hoyos RE, Sarafidis V. Testing for cross-sectional dependence in panel-data models. STATA J. 2006;6(4):482–96.
Pesaran MH. Estimation and inference in large heterogeneous panels with a multifactor error structure. Econometrica. 2006;74(4):967–1012.
Pesaran MH. A simple panel unit root test in the presence of cross-section dependence. J ApplEconomet. 2007;22(2):265–312.
Breusch TS, Pagan AR. The Lagrange multiplier test and its applications to model specification in econometrics. Rev Econ Stud. 1980;47(1):239–53.
Pesaran MH. General diagnostic tests for cross-section dependence in panels. UK: IZA Discussion Paper No. 1240, University of Cambridge; 2004.
Book Google Scholar
Baltagi BH, Feng Q, Kao C. A Lagrange Multiplier test for cross-sectional dependence in a fixed effects panel data model. J Econometrics. 2012;170(1):164–77.
Tugcu CT, Tiwari AK. Does renewable and/or non-renewable energy consumption matter for total factor productivity (TFP) growth? Evidence from the BRICS. Renew Sust Energ Rev. 2016;65:610–6.
Friedman M. The use of ranks to avoid the assumption of normality implicit in the analysis of variance. J Am Stat Assoc. 1937;32(200):675–701.
Frees EW. Assessing cross-sectional correlation in panel data. J Econometrics. 1995;69:393–414.
Frees EW. Longitudinal and panel data: analysis and applications in the social sciences. Illustrated ed. Cambridge: Cambridge University Press; 2004.
Im KS, Pesaran MH, Shin Y. Testing for Unit Roots in Heterogeneous Panels. J Econometrics. 2003;115(1):53–74.
Maddala GS, Wu S. A comparative study of unit root tests with panel data and a new simple test. Oxford B Econ Stat. 1999;61(S1):631–52.
Choi I. Unit root tests for panel data. J Int Money Finance. 2001;20:249–72.
Levin A, Lin CF, Chu CSJ. Unit root tests in panel data: asymptotic and finite-sample properties. J Econometrics. 2002;108(1):1–24.
Breitung J. The local power of some unit root tests for panel data. In: B. Baltagi (ed.), Nonstationary Panels, Panel Cointegration, and Dynamic Panels. Adv Econom. 2000;15(JAI):161–178.
Hadri K. Testing for stationarity in heterogeneous panel data. Economist J. 2000;3(2):148–61.
Bai J, Ng S. A panic attack on unit roots and Cointegration. Econometrica. 2004;72:1127–77.
Chang Y, Non-linear IV. Unit root tests in panels with cross-sectional dependency. J Econometrics. 2002;110:261–92.
Chang Y. Bootstrap unit root tests in panels with cross-sectional dependency. J Econometrics. 2004;120:263–93.
Choi I. Combination unit root tests for cross-sectionally correlated panels. 2002.
Phillips PCB, Sul D. Dynamic panel estimation and homogeneity testing under cross section dependence. Economist J. 2003;6:217–59.
Harris R, Sollis R. Applied time series modeling and forecasting. 1st ed. Hoboken, New Jersey: Wiley; 2003.
Smith LV, Leybourne S, Kim TH, Newbold P. More powerful panel data unit root tests with an application to mean reversion in real exchange rates. J ApplEconomet. 2004;19(2):147–70.
Moon HR, Perron B. Testing for unit root in panels with dynamic factors. J Econometrics. 2004;122:81–126.
Cerrato M, Sarantis N. A bootstrap panel unit root test under cross-sectional dependence, with an application to PPP. Comput Stat Data An. 2007;51(8):4028–37.
Palm FC, Smeekes S, Urbain JP. Cross-sectional dependence robust block bootstrap panel unit root tests. J Econometrics. 2011;163(1):85–104.
O’Connell PGJ. The overvaluation of purchasing power parity. J Int Econ. 1998;44:1–19.
Hurlin C, Mignon V. Une Synthèse des Tests de Racine Unitaire sur Données de panel. Economie et Prévision. 2005;3–4(169):253–94.
Baltagi BH. Econometric Analysis of Panel Data. 3rd ed. Chichester: John Wiley & Sons; 2008.
Chudik A, Pesaran MH. Large panel data models with cross-sectional dependence: a survey. In: Baltagi BH, editor. The Oxford Handbook of panel data. New York: rd University Press; 2015. p. 3–45.
Chapter Google Scholar
Eberhardt M, Presbitero AF. Public debt and growth: Heterogeneity and non-linearity. J Int Econ. 2015;97(1):45–58.
Hashiguchi Y, Hamori S. Small sample properties of CIPS panel unit root test under conditional and unconditional heteroscedasticity. 2010. MPRA Paper No. 24053. Available from: https://mpra.ub.uni-muenchen.de/24053/ .
Choi I. Unit root tests for cross-sectionally correlated panels. In: Econometric theory and practice: frontiers of analysis and applied research. 2006.
Albulescu CT, Pépin D, Tiwari AK. A re-examination of real interest parity in CEECs using ‘old’ and ‘new’ second-generation panel unit root tests. B Econ Res. 2016;68(2):133–50.
Westerlund J. Testing for error correction in panel data. Oxford B Econ Stat. 2007;69(6):709–48.
Westerlund J, Edgerton DL. A panel bootstrap cointegration test. Econ Lett. 2007;97(3):185–90.
Westerlund J, Edgerton DL. A simple test for cointegration in dependent panels with structural breaks. Oxford B Econ Stat. 2008;70(5):665–704.
Groen JJJ, Kleibergen F. Likelihood-based cointegration analysis in panels of vector error-correction models. J Bus Econ Stat. 2003;21(2):295–318.
Westerlund J. Panel cointegration tests of the Fisher effect. J ApplEconomet. 2008;23(2):193–233.
Gengenbach C, Urbain JP, Westerlund J. Error correction testing in panels with common stochastic trends. J ApplEconomet. 2016;31(6):982–1004.
Banerjee A, Carrion-i-Silvestre JL. Testing for panel cointegration using common correlated effects estimators. J Time Ser Anal. 2017;38(4):610–36.
McCoskey S, Kao C. A residual-based test of the null of cointegration in panel data. Economet Rev. 1998;17(1):57–84.
Banerjee A, Dolado J, Mestre R. Error-correction mechanism tests for cointegration in a single-equation framework. J Time Ser Anal. 1998;19(3):267–83.
Abdullah SM, Siddiqua S, Huque R. Is health care a necessary or luxury product for Asian countries? An answer using the panel approach. Heal Econ Rev. 2017;7(1):1–12.
Martins PM. Aid absorption and spending in Africa: a panel cointegration approach. J Dev Stud. 2011;47(12):1925–53.
Pedroni P. Critical values for cointegration tests in heterogeneous panels with multiple regressors. Oxford B Econ Stat. 1999;61:653–70.
Pedroni P. Panel cointegration: asymptotic and finite sample properties of pooled time series tests with an application to the PPP hypothesis. Economet Theor. 2004;20(3):597–625.
Kao C. Spurious regression and residual-based tests for cointegration in panel data. J Econometrics. 1999;90:1–44.
Beyene SD. Kotosz B Testing the environmental Kuznets curve hypothesis: an empirical study for East African countries. Int J Environ Stud. 2020;77(4):636–54.
Driscoll JC, Kraay AC. Consistent covariance matrix estimation with spatially dependent panel data. Rev Econ Stat. 1998;80(4):549–60.
Hoechle D. Robust standard errors for panel regressions with cross-sectional dependence. STATA J. 2007;7(3):281–312.
Breitung J, Pesaran MH. Unit roots and cointegration in panels. In: The econometrics of panel data. Berlin, Heidelberg: Springer; 2008.
Firebaugh G, Warner C, Massoglia M. Fixed effects, random effects, and hybrid models for causal analysis. In: Morgan S, editor. Handbook of causal analysis for social research. Dordrecht: Springer; 2013. p. 113–32.
Allard A, Takman J, Uddin GS, Ahmed A. The N-shaped environmental Kuznets curve: an empirical evaluation using a panel quantile regression approach. Environ SciPollut Res. 2018;25(6):5848–61.
Bayar Y, Odabas H, Sasmaz MU, Ozturk OF. Corruption and shadow economy in transition economies of European Union countries: a panel cointegration and causality analysis. Econ Res-Ekon Istraz. 2018;31(1):1940–52.
Barbieri L. Panel Cointegration Tests: A Survey. Rivista Internazionale Di Scienze Sociali. 2008;116(1):3–36.
Kao C, Chiang MH. On the estimation and inference of a cointegrated regression in panel data. In Baltagi BH, Fomby TB, Hill RC (Ed.) Nonstationary panels, panel cointegration, and dynamic panels (Advances in Econometrics, Vol. 15, pp.179–222). Bingley: Emerald Group Publishing Limited; 2001.
Roodman D. How to do xtabond2: an introduction to difference and system GMM in Stata. Stand Genomic Sci. 2009;9(1):86–136.
Eslamloueyan K, Jokar Z. Energy consumption and economic growth in the Middle East and north Africa: a multivariate causality test. Iran J Econ Stud. 2014;18(57):27–46.
CrunchEconometrix. Econometrics and Data Analysis Resources: (Stata13): How to Generate Long-run GMM Coefficients. 2022. Available from: https://www.youtube.com/watch?v=01wUyHVZnTY&ab_channel=CrunchEconometrix
Dumitrescu EI, Hurlin C. Testing for granger non-causality in heterogeneous panels. Econ Model. 2012;29(4):1450–60.
Cohen J. Statistical Power Analysis for the Behavioural Sciences. 2nd ed. New York: Psychology Press; 1988.
Hansen LP. Large sample properties of generalized method of moments estimators. Econometrica. 1982;50(4):1029–54.
Sargan JD. The estimation of economic relationships using instrumental variables. Econometrica. 1958;26(3):393–415.
FAO, IFAD, UNICEF, WFP, WHO The State of Food Security and Nutrition in the World. Transforming Food Systems to Deliver Affordable Healthy Diets for All FAO. 2020. Available from: https://www.fao.org/publications/sofi/2020/en/ .
Van Ittersum MK, Van Bussel LG, Wolf J, Grassini P, Van Wart J, Guilpart N, Claessens L, De Groot H, Wiebe K, Mason-D’Croz D, Yang H. Can sub-Saharan Africa feed itself? Proce Natl Acad Sci. 2016;113(52):14964–9.
Global Nutrition Report. Country Nutrition Profiles. 2021. https://globalnutritionreport.org/resources/nutrition-profiles/africa/ .
Herrero M, Thornton PK, Power B, Bogard JR, Remans R, Fritz S, Gerber JS, Nelson G, See L, Waha K, Watson RA. Farming and the geography of nutrient production for human use: a transdisciplinary analysis. Lancet Planet Health. 2017;1(1):e33-42.
Sibhatu KT, Qaim M. Rural food security, subsistence agriculture, and seasonality. PLoS ONE. 2017;12(10): e0186406.
Fanzo J. The role of farming and rural development is central to our diets. Physiol Behav. 2018;193:291–7.
Download references
Acknowledgements
The author sincerely thanks the Editor, the three anonymous reviewers, and BalázsKotosz (Adjunct Professor) for their comments and advice.
This study did not receive any specific grant.
Author information
Authors and affiliations.
College of Business and Economics, Department of Economics, Arsi University, Asella, Ethiopia
Sisay Demissew Beyene
You can also search for this author in PubMed Google Scholar
Contributions
SDB collected, analyzed, and interpreted the data, and wrote and approved the paper for submission.
Corresponding author
Correspondence to Sisay Demissew Beyene .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Competing interests.
The author declares that there are no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:.
Table S1. Cook’s D results
Additional file 2:
Table S2. Hausman and Breusch-Pagan LM for REtests.
Additional file 3.
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Beyene, S.D. The impact of food insecurity on health outcomes: empirical evidence from sub-Saharan African countries. BMC Public Health 23 , 338 (2023). https://doi.org/10.1186/s12889-023-15244-3
Download citation
Received : 07 March 2022
Accepted : 08 February 2023
Published : 15 February 2023
DOI : https://doi.org/10.1186/s12889-023-15244-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Food insecurity
- Life expectancy
- Infant mortality
- Panel data estimations
- SSA countries
BMC Public Health
ISSN: 1471-2458
- General enquiries: [email protected]
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 31 October 2022
Food insecurity
Nature Climate Change volume 12 , page 963 ( 2022 ) Cite this article
7387 Accesses
3 Citations
25 Altmetric
Metrics details
- Agriculture
- Climate-change impacts
Climate change is a confounding factor that can affect agriculture and food security in many different ways. Climate-resilient food systems are needed to ensure food security and to support mitigation efforts.
World Food Day — 16 October, with the theme this year of ‘leave no one behind’ — is an appropriate time to reflect on global progress toward Sustainable Development Goal 2: Zero Hunger. The 2022 Global Hunger Index, released October 2022 ( https://www.globalhungerindex.org/ ), highlights that progress has stagnated, with the war in Ukraine, climate change and related extreme events, and the related increased price of food, fuel and fertilizer all contributing. The 2022 Global Hunger Index report 1 highlights that 44 countries are currently suffering serious or alarming levels of hunger, although there is large within-country variability. The report estimates that 828 million people are currently undernourished, with parts of Africa south of the Sahara and South Asia having the highest hunger levels, and being the most vulnerable to future shocks.

Climate change can affect crops in different ways and the impacts of climate change due to higher levels of atmospheric CO 2 are often deleterious. While higher levels of atmospheric CO 2 may enhance photosynthesis and growth in some crops 2 , there isn’t a clear picture on the overall effects on crops. Further, it has been reported that plants grown under higher CO 2 levels have changed nutritional value 3 .
Warming temperatures due to climate change also impact crop productivity, with an example discussed in this issue of Nature Climate Change . In an Article , Peng Zhu and colleagues consider how warming temperatures affect cropping frequency and yields. They find that warmer temperatures are increasing productivity and the possibility of multiple cropping seasons in cold regions, but increased temperatures in warm regions are causing decreases that outweigh the cold-region increases for an overall loss in crop productivity. The authors note that irrigation can offset the losses in warm regions, but water availability and the infrastructure needed suggest that the required 5% expansion of irrigation areas would be difficult to achieve.
Research has highlighted the risks of concurrent regional droughts; for example, work looking at 26 main crop-producing countries that found the probability under a high-emissions scenario to be at least 5% compared with 0% in the historical period 4 , as well as work showing increases by 40–60% for 10 global regions, with disproportionate risk increase across North America and the Amazon region 5 . With many regions relying on rain-fed agriculture, drought is a major risk to crop failure.
The shifting of seasons, in particular wet periods, can also affect planting. The northern USA had heavy spring rains this year that limited corn planting. This reduced planting led the US Department of Agriculture to lower the predicted yield per acre by 4 bushels, which equals more than 9 million tonnes less corn crop across the country. This lower yield, alongside lower-than-expected grain harvests in China, India, South America and part of Europe, reduced the available produce, not only for consumption but also for stock feed.
As well as their impact on production, extreme events can be a major disruption of supply chains. Yet, international trade has been highlighted as a possible way to mitigate climate change impacts on food security. It has been shown that high-emissions climate scenarios lead to increased hunger risk of 33–47% when trade is restricted, but decreases to 11–64% when trade is open 6 . However, production for export does need to be carefully considered to minimize negative effects in the producing region 7 .
The need to transform food systems to ensure resilience to climate change and other external pressures is well recognized, yet in climate change discussions it has not always been at the fore; at COP27, there will be a Food Systems Pavilion for the first time. How to achieve food systems transformation needs careful consideration and discussion, but work needs to begin now to push past the current stagnation and to ensure that no one is left behind.
von Grebmer, K. et al. 2022 Global Hunger Index: Food Systems Transformation and Local Governance (Welthungerhilfe, Concern Worldwide, 2022).
Toreti, A. et al. Nat. Food 1 , 775–782 (2020).
Article CAS Google Scholar
Dong, J., Gruda, N., Lam, S. K., Li, X. & Duan, Z. Front. Plant Sci. https://doi.org/10.3389/fpls.2018.00924 (2018).
Article Google Scholar
Qi, W., Feng, L., Yang, H. & Liu, J. Geophys. Res. Lett. 49 , e2021GL097060 (2022).
Google Scholar
Singh, J. et al. Nat. Clim. Change 12 , 163–170 (2022).
Janssens, C. et al. Nat. Clim. Change 10 , 829–835 (2020).
The State of Food Security and Nutrition in the World 2022. Repurposing Food and Agricultural Policies to Make Healthy Diets More Affordable (FAO, IFAD, UNICEF, WFP, WHO, 2022); https://doi.org/10.4060/cc0639en
Download references
Rights and permissions
Reprints and permissions
About this article
Cite this article.
Food insecurity. Nat. Clim. Chang. 12 , 963 (2022). https://doi.org/10.1038/s41558-022-01530-2
Download citation
Published : 31 October 2022
Issue Date : November 2022
DOI : https://doi.org/10.1038/s41558-022-01530-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Feeding the future world.
Nature Climate Change (2024)
Interactions between an arbuscular mycorrhizal inoculum and the root-associated microbiome in shaping the response of Capsicum annuum “Locale di Senise” to different irrigation levels
- Alice Calvo
- Thomas Reitz
- Raffaella Balestrini
Plant and Soil (2024)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing: Anthropocene newsletter — what matters in anthropocene research, free to your inbox weekly.

Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Journal Menu
- Aims & Scope
- Editorial Board
- Reviewer Board
- Topical Advisory Panel
- Instructions for Authors
- Special Issues
- Sections & Collections
- Article Processing Charge
- Indexing & Archiving
- Editor’s Choice Articles
- Most Cited & Viewed
- Journal Statistics
- Journal History
- Journal Awards
- Society Collaborations
- Conferences
- Editorial Office
Journal Browser
- arrow_forward_ios Forthcoming issue arrow_forward_ios Current issue
- Vol. 13 (2024)
- Vol. 12 (2023)
- Vol. 11 (2022)
- Vol. 10 (2021)
- Vol. 9 (2020)
- Vol. 8 (2019)
- Vol. 7 (2018)
- Vol. 6 (2017)
- Vol. 5 (2016)
- Vol. 4 (2015)
- Vol. 3 (2014)
- Vol. 2 (2013)
- Vol. 1 (2012)
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
Food Insecurity: Causes, Consequences and Remedies
- Print Special Issue Flyer
- Special Issue Editors
Special Issue Information
Benefits of publishing in a special issue.
- Published Papers
A special issue of Foods (ISSN 2304-8158). This special issue belongs to the section " Food Security and Sustainability ".
Deadline for manuscript submissions: closed (31 October 2023) | Viewed by 31338
Share This Special Issue
Special issue editor.

Dear Colleagues,
Food insecurity affects all communities worldwide as many find it difficult to consistently access nutritious, affordable food. This problem is exacerbated by conflict, political insecurity, climate change, and global shocks such as the COVID-19 pandemic.
This Special Issue seeks to develop a collection of innovative, contemporary research that considers the causes, consequences and remedies for food insecurity at an individual, household, community, regional, or even global scale. Multiple socio-economic factors influence food insecurity, particularly nutrition insecurity; these will be explored within the research papers, alongside the contemporary politico-environmental factors that also play a part.
This Special Issue welcomes contributions from researchers across the world who are considering how to address food insecurity and what mechanisms are of the greatest benefit in reaching the sustainable development goals, especially SDG1: no poverty; SDG 2: zero hunger; SDG 3: good health and wellbeing, and SDG 10: reducing inequalities.
Prof. Dr. Louise Manning Guest Editor
Manuscripts should be submitted online at www.mdpi.com by registering and logging in to this website . Once you are registered, click here to go to the submission form . Manuscripts can be submitted until the deadline. All submissions that pass pre-check are peer-reviewed. Accepted papers will be published continuously in the journal (as soon as accepted) and will be listed together on the special issue website. Research articles, review articles as well as short communications are invited. For planned papers, a title and short abstract (about 100 words) can be sent to the Editorial Office for announcement on this website.
Submitted manuscripts should not have been published previously, nor be under consideration for publication elsewhere (except conference proceedings papers). All manuscripts are thoroughly refereed through a single-blind peer-review process. A guide for authors and other relevant information for submission of manuscripts is available on the Instructions for Authors page. Foods is an international peer-reviewed open access semimonthly journal published by MDPI.
Please visit the Instructions for Authors page before submitting a manuscript. The Article Processing Charge (APC) for publication in this open access journal is 2900 CHF (Swiss Francs). Submitted papers should be well formatted and use good English. Authors may use MDPI's English editing service prior to publication or during author revisions.
- food security
- food insecurity
- consequences
- self-sufficiency
- Ease of navigation: Grouping papers by topic helps scholars navigate broad scope journals more efficiently.
- Greater discoverability: Special Issues support the reach and impact of scientific research. Articles in Special Issues are more discoverable and cited more frequently.
- Expansion of research network: Special Issues facilitate connections among authors, fostering scientific collaborations.
- External promotion: Articles in Special Issues are often promoted through the journal's social media, increasing their visibility.
- e-Book format: Special Issues with more than 10 articles can be published as dedicated e-books, ensuring wide and rapid dissemination.
Further information on MDPI's Special Issue polices can be found here .
Published Papers (10 papers)
Jump to: Review , Other
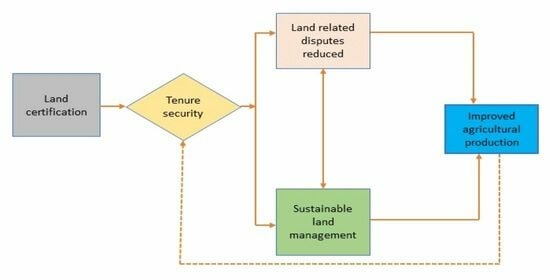
Graphical abstract
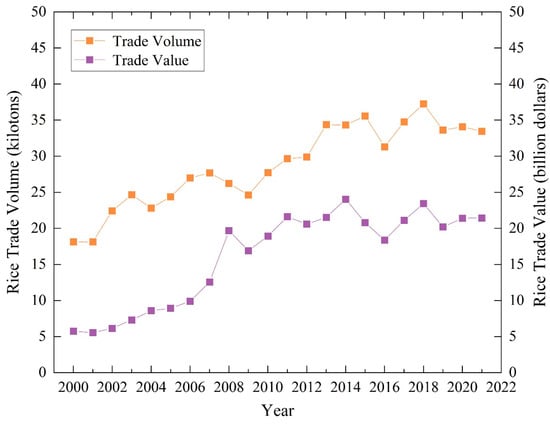
Jump to: Research , Other

Jump to: Research , Review
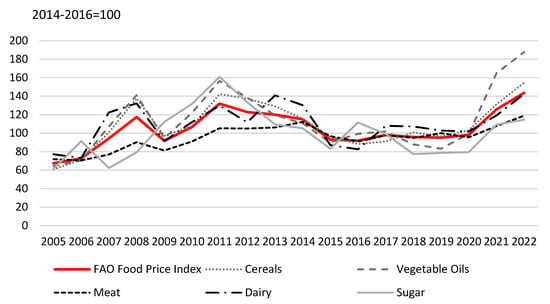
Further Information
Mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
- Nutrition and Dietetics
- Food Insecurity
Food Insecurity: Concept, Causes, Effects and Possible Solutions
- November 2021
- 2(1):105-113

- Aligarh Muslim University

Discover the world's research
- 25+ million members
- 160+ million publication pages
- 2.3+ billion citations

- Alyandani Ayu Kinanti

- Tolulope R. Jerumeh
- Altaf Ghani
- Hassam Ahmad Hashmi
- Ezra Chitando

- Angela D Liese

- Nicholas Sambanis
- Kevin Watkins
- G.A. Epstein
- FUTURE CHILD
- Craig Gundersen

- Recruit researchers
- Join for free
- Login Email Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google Welcome back! Please log in. Email · Hint Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google No account? Sign up

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Increasing Access to Healthy Foods through Improving Food Environment: A Review of Mixed Methods Intervention Studies with Residents of Low-Income Communities
Associated data.
Not applicable.
Food insecurity is a broad and serious public health issue in the United States, where many people are reporting lack of access to healthy foods. The reduced availability of healthy, affordable foods has led to increased consumption of energy-dense and nutrient-poor foods, resulting in increasing the risk for many chronic diseases such as obesity, cardiovascular diseases, and type 2 diabetes mellitus. Thus, identifying promising approaches to increase access to healthy foods through improving the food environment is of importance. The purpose of this review article is to highlight how the food environment affects directly a person’s food choices, and how to increase access to healthy foods through improving environmental approaches. The literature search was focused on finding different approaches to improve food security, primarily those with an impact on food environment. Overall, potential solutions were gathered through multilevel environmental approaches, including nutrition education and peer education, community-based participatory research, and policy changes in supplemental nutrition programs. A recommendation to reduce food insecurity is learning to create meals with a variety of seasonal fruits and vegetables purchased from affordable farmers’ markets.
1. Introduction
Food insecurity comprises limited or uncertain access to nutritious and adequate food intake and is widespread in the United States [ 1 ]. The United States Department of Agriculture (USDA) reported that 10.5% of Americans were food insecure at least some of the time during 2019 [ 2 ]. Many individuals who are food insecure utilize food banks and food pantries to procure food, but studies have shown that pantry users consume limited amounts of fruits, vegetables, and fiber [ 3 ]. The majority of the calories for this population are taken from energy-dense, nutrient-poor foods, including refined grains and foods high in added sugars and saturated fats, in contrast with the food-secure population, who have access to more nutrient-dense and healthier options [ 4 ]. This can result in the consumption of empty calories, rather than insufficient calories [ 4 ]. In general, food-secure individuals are more likely to meet the recommended dietary allowance for nutrients than food-insecure individuals [ 5 ]. This is displayed in a study by Champagne et al. [ 5 ], in which researchers determined the food security status through self-reported food intake, and found that food insecurity is associated with lower-quality diets assessed by the healthy eating index (HEI) scores.
A few factors that affect poor diet quality are related to lack of access to healthy foods in the surrounding neighborhood and limited household income [ 3 , 6 ]. The macro-environmental sector refers to broad infrastructure (including food advertising and health systems), whereas micro-environments indicate local settings (such as workplaces and homes) [ 7 ]. Through improving these food environments, access to healthy food options can be increased, resulting in better diet quality and reduced chronic disease risk in these populations. Therefore, developing effective strategies to improve the diet quality and nutritional status of high-risk populations is important for the prevention of diet-related chronic disease. This review paper will evaluate specific risks for chronic disease associated with food insecurity and strategies to improve the food environment and individuals’ choices towards a healthier diet and lifestyle. The objectives will be reached through assessing the literature on mixed-method intervention studies with residents of low-income communities.
2. Materials and Methods
To learn more about food insecurity and the risk of chronic disease, as well as approaches to improve food access, a literature search was conducted in June 2021 using the databases PubMed, Scopus, and Google Scholar, with a combination of keywords “food insecurity”, “chronic disease”, “food access”, “multilevel approaches”, “low-income”, “healthy eating”, “community”, and “policy changes”. Reading through each study, the titles and abstracts were observed to identify which articles provided informative data that helped towards reducing food insecurity. As summarized in Table 1 , full-length articles and book chapters in English with the US population in focus for all age ranges were selected. There were no limits to the state or region in the US in which the studies were conducted. The study designs conducted were randomized controlled trials, clinical trials, comparative studies, multicenter studies, and cohort studies. Notes, comments, editorials, and review articles were excluded from the articles with an exception of two review articles that were complementary to the data from other major studies. Studies that had other populations in focus, including low-income communities outside of the US, were excluded. Additionally, there were studies selected from the reference lists of relevant articles. Studies that compared the lifestyle and diet of food-secure populations vs. food-insecure populations were included, with a specific focus on the impact of the food environment. As different approaches to improve food security were searched for this narrative review, there was a focus on nutrition and peer education, community-based research, policy changes, and multilevel approaches.
Criteria for studies included.
| Parameter | Criteria | Exclusion |
|---|---|---|
| Search terms included | Food insecurity, chronic disease, multilevel approaches, low-income, food environment. | N/A |
| Criteria for study design | RCT, clinical trials, comparative studies, multicenter studies, cohort studies, qualitative studies, books. | Review articles, notes, comments, editorials. |
| Criteria for subject population | Low-income populations, all age ranges. | Other populations, low-income population not living in US. |
| Criteria for outcomes | Improved dietary behavior, weight status, improved lifestyle, educating the community on healthier choices when on a budget. | N/A |
3. Food Insecurity and Risk for Diet-Related Chronic Disease
3.1. obesity.
At the individual level, rates of obesity are higher among groups with low education and low incomes [ 8 , 9 ]. Current meta-analysis studies show that food insecurity increases the risk for obesity for adults (odds ratio 1.15) in food-insecure households, especially women odds ratio of 1.26) [ 10 ]. Paeratakul et al. [ 9 ] assessed data from the USDA Agricultural Research Service Continuing Survey of Food Intakes by Individuals, and reported that, among other factors, socioeconomic condition is one of the main factors leading to greater obesity severity. The study further linked obesity rates with an increased incidence of diabetes, hypertension, and high serum cholesterol, which further supports the role of socioeconomic factors in increasing these disease risks through an increase in obesity [ 9 ]. Individuals with food insecurity commonly use resources, such as food pantries, for access to a variety of products. An important issue that has been shown to lead to obesity among low-income populations is the poor nutritional quality of food and lack of knowledge of how to prepare certain fresh produce provided by the food pantries and other food assistance programs [ 5 , 11 ]. A great focus has been towards children in low-income populations and their greater risk of obesity due to their diet patterns and food choices [ 12 ]. Kaur et al. [ 12 ] analyzed the National Health and Nutrition Examination Survey (NHANES) data assessing personal food insecurity through USDA’s Food Security Survey Module to determine its relationship with obesity risk. The researchers determined that obesity was significantly associated with levels of food insecurity among children of ages 6 to 11 years, with an odds ratio of 1.81; 95% confidence interval (CI) 1.33 to 2.48 [ 12 ].
Food pantries are good resources from which to analyze the needs of food-insecure populations and determine obesity rates. Studies of food pantry participants concluded that the mean body mass index (BMI) of the pantry users was 29.5 kg/m 2 , and 78.0% of the population of obese pantry users were women [ 3 , 5 , 11 , 13 ]. Many people from the population have shown an interest in regularly consuming nutritious food and fresh produce, but they reported that these products were unaffordable [ 14 , 15 ].
3.2. Cardiovascular Diseases
According to the American Heart Association, the seven cardiovascular health metrics are based on smoking, diet, physical activity, BMI, blood pressure, total cholesterol, and fasting glucose [ 16 ]. Individuals with food insecurity face barriers meeting the ideal cardiovascular health metrics, including lower odds of meeting at least three metrics ( p < 0.01) [ 17 ]. Data further show a greater presence of hypertension and heart disease in individuals with lower education and income compared to others [ 9 ]. Furthermore, hypertension is associated with greater intake of added sugar and sugar-sweetened beverages ( p < 0.05) [ 18 ]. Adults from food-insecure households had a 21% higher risk of clinical hypertension than adults from food-secure households [ 19 ]. A systemic review and meta-analysis of 36 studies indicated an association between food-insecure adults and self-reported hypertension with an odds ratio of 1.13 [ 20 ]. Additionally, very low food security was associated with increased risk for cardiovascular disease, and a 58% higher risk for cardiovascular disease mortality [ 21 , 22 , 23 ]. Sun et al. focused on associations of adult food insecurity with all-cause and cardiovascular disease mortality in US adults [ 23 ]. This study concluded that participants with very low food security had a higher risk of cardiovascular disease compared with those with high food security, with an odds ratio of 1.54 (95% CI 1.04–2.26) [ 23 ].
Bazzano et al. [ 24 ] conducted the first NHANES Follow-up Study to observe fruit and vegetable intake through a food-frequency questionnaire, and the incidence of mortality from cardiovascular disease from medical records and death certificates. A significant association was identified between frequency of fruit and vegetable intake and incidence of and mortality from stroke, ischemic heart disease, and cardiovascular disease [ 24 ]. Bazzano et al. [ 24 ] further concluded that consuming three or more fruits and vegetables per day, compared to less than one per day, was associated with a 27% lower stroke incidence, a 42% lower stroke mortality, a 24% lower ischemic heart disease mortality, a 27% lower cardiovascular disease mortality, and a 15% lower all-cause mortality. Due to the high cost of fruits and vegetables, lack of transportation, low quality products in low-income areas, and other factors, individuals in these neighborhoods consume fewer servings of fruits and vegetables than the Dietary Guidelines recommendations, leading to an increased risk for cardiovascular disease [ 25 ]. Among nonelderly adults with household income <200% of the federal poverty level, analysis of NHANES data by Seligman et al. [ 19 ] (a nationally representative survey of the US population) found an association between food insecurity and clinical evidence of hypertension and diabetes.
3.3. Diabetes Mellitus
As previously mentioned, poor diet quality includes low nutrient consumption and high intake of energy dense foods. This lifestyle factor is one of the main factors leading to diabetes mellitus. Walker et al. [ 13 ] conducted a cross-sectional analysis with data from the NHANES survey 2005–2014 to evaluate levels of food security and its association to diabetes. The results indicated higher risk for food insecurity, with an odds ratio for prediabetes of 1.39 (95% CI 1.21–1.59), for undiagnosed diabetes of 1.81 (95% CI 1.37–2.38), and for diagnosed diabetes of 1.58 (95% CI 1.29–1.93) [ 13 ]. The results are supported by a cross-sectional study; when compared to individuals with food security, participants with low food security were 1.35 times more likely to have prediabetes (95% CI: 1.17–1.55) [ 26 ]. Very-low-food-secure participants, compared with both low-food-secure and food-secure participants, have been reported to have greater diabetes distress and more frequent and severe hypoglycemic episodes [ 27 ]. Individuals with food insecurity live paycheck by paycheck or wait for monthly assistance, which can lead to a cycle of restraining dietary intake during hard times and overeating during food restock [ 28 ]. This process can lead to insulin resistance and diabetes [ 13 , 28 , 29 ]. In individuals with food security the self-management to improve diabetes is easier, but a lack of quality food makes diabetes self-management more difficult, worsening the food-insecure individual’s health condition [ 27 ]. A meta-analysis study by Abdurahman et al. further strengthens the hypothesis for an association between household food insecurity and increased risk of type 2 diabetes, with an odds ratio value of 1.27 (95% CI 1.11–1.42) [ 30 ]. Based on the studies mentioned previously, it appears that food insecurity is associated with different stages of diabetes mellitus; however, there are some recent studies that contrast the findings and do not suggest an association between food insecurity and clinically determined type 2 diabetes or significant differences in fasting blood glucose and HbA1c [ 31 ]. Beltran et al. additionally stated that food insecurity is a complex issue and it might look different depending on factors such as social, economic, and geographic consideration [ 31 ]. The study explained that the differences in the findings might be a result of the difference in food insecurity concepts, where in some cases hunger and chronic starvation are the primary drives of food insecurity [ 31 ]. In another study, starvation due to food insecurity was related to worsening signs of insulin sensitivity in type 2 diabetes [ 29 ]. Meanwhile, food-insecure areas in the United States are usually not associated with hunger, but mainly with intake of lower-quality, high-calorie foods, which increase a person’s risk for type 2 diabetes [ 31 ].
4. The Impact of Food Environment on Access to Healthy Food Choices
The nutritional environment is affected not only by the number of stores in an area but also the availability and cost of healthy food items. Reduced access to fresh produce greatly impacts food choices for low-income populations [ 32 ]. Typically, individuals with reliable transportation make frequent trips to supermarkets [ 32 , 33 ]. However, many people in low-income neighborhoods rely greatly on food pantries due to the lack of transportation and availability of fresh produce in their areas [ 33 ]. A research study, conducted in a low-income neighborhood in Pomona, CA, determined that 41% of the food pantry clients did not live within walking distance of a store with a variety of fresh produce and 13% did not have access to any type of food store with fresh produce [ 33 ]. This problem is widespread in many areas in the US and highlights rural adults not being able to meet recommended nutrition guidelines due to environmental barriers and lack of community resources [ 33 ]. In areas with food insecurity, convenience stores are more common than supermarkets or grocery stores [ 32 ]. These stores have a very limited range of food items and are more likely to stock less healthy versions of products (for example: low-fiber bread vs. high-fiber bread, whole milk vs. reduced-fat milk vs. low-fat or nonfat milk) [ 32 ]. A multicenter study in Hartford, CT, combined customer shopping behavior with store food inventory data, and concluded that when there is a greater variety of fresh products, such as fruits and vegetables, there is an increased likelihood of these products being purchased [ 34 ]. This research study conducted face-to-face interviews on different days and at different times of the day to measure typical food shopping behaviors and determine whether shoppers had access to and used the Supplemental Nutrition Assistance Program (SNAP) and Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) benefits in the store [ 34 ]. They also maintained inventories, using a modified version of the Nutrition Environment Measures Survey in Stores (which included the availability of fresh/canned fruits and vegetables, and whole grain and reduced-fat dairy products) to measure availability and quality of healthy food in stores [ 34 ]. Due to an increased variety of fruits and vegetables offered, those receiving SNAP were significantly more likely to purchase fruit ( p < 0.05) and vegetables ( p < 0.01), compared with those who were not receiving SNAP [ 34 ].
When it comes to the cost of fresh products, more healthful versions of food items are typically more expensive than the corresponding less-healthful versions, with the exception of milk [ 35 ]. At the same time, foods with high energy density provide the most calories at a lower cost, which contributes to people in low-income populations consuming them over fresh, nutrient-dense products [ 35 ]. Alteration of this environment, as with the study discussed above by Martin et al. [ 34 ], may significantly change these consumption habits.
5. Environmental Approaches to Improve Food Security and Nutritional Status: Multilevel Intervention Studies with Residents of Low-Income Communities
Figure 1 uses the framework of the socioecological model (SEM) concept, as outlined by the Centers for Disease Control and Prevention [ 36 ], to summarize the key multilevel approaches discussed in this review for improving food security and nutritional status. Environmental approaches and nutrition programs can improve food security more efficiently if they work in a multilevel interaction approach [ 36 ]. This interaction starts from working personally with the individual, to creating a support system of family, friends, and social networks [ 36 ]. Other more significant factors that can assist this population are resources provided through schools or workplaces, communities (considering cultural values and norms), and policy changes from local laws to national changes [ 36 ]. Multilevel approaches have been used to increase the fruit and vegetable intake in low-income housing communities. Table 2 summarizes the key approaches that have led to improvements in food security. A 12-month cluster, randomized controlled trial (RCT) was conducted to demonstrate the benefit of year-round fruit and vegetable markets at improving fruit and vegetable (F&V) intake for low-income adults [ 37 ]. This research study featured discount fresh fruit and vegetable markets called ‘Fresh to You’ (FTY), as well as a multicomponent, educational intervention, which was a combination of individual, community, and policy change approaches [ 37 ]. The prices of the fruits and vegetables were kept at or below the retail prices at local supermarkets [ 37 ]. This study also included chef-run cooking demonstrations, taste-testing events, shared recipes, and educational boxes (including newsletters, DVDs, reusable shopping bags, and kitchenware) and two six-week educational/motivational campaigns, which focused on increasing intake and variety of fruits and vegetables [ 37 ]. The results indicated that more than half of the participants attended a few of the FTY markets [ 37 ]. From baseline to 12 months, there was an increase in total fruit and vegetable intake by 0.44 cup/day (as assessed by the National Cancer Institute’s ‘Eating at America’s Table All Day Screener’) in the intervention group with the control group decreasing intake by 0.08 cup/day [ 37 ]. There was also an increase in the frequency of fruits and vegetables by 0.24 servings per day, which was assessed through the Fruit and Vegetable Habits Questionnaire Score [ 37 ]. Reading newsletters or attending campaign events was not associated with any change in fruit and vegetable consumption, but watching DVDs was associated with an increase in fruit and vegetable intake by 0.69 cup/day [ 37 ].
Summary of key studies to increase access to healthy foods.
| Author | Type of Study | Target Population | Sample Size | Type of Approach | Outcome Measure | Results |
|---|---|---|---|---|---|---|
| Gans. et al. [ ] | RCT | Western adults | 1587 | Individual, community, policy Changes | Fruit and vegetable consumption measured by National Cancer Institute’s “Eating at America’s Table All Day Screener” | -↑ total intake F & V by 0.44 c/day with the control group ↓ by 0.08 c/day ( < 0.02). -↑ F&V frequency ( = 0.01) |
| Trude. et al. [ ] | RCT | Obese children (9–15 years old) in 30 areas of Baltimore. | 401 | Individual, interpersonal, organizational, community, policy | -Purchase and consumption of low-sugar foods and beverages. | -↑ healthier purchases by 1.4 more items per week compared to the control group. -There was a 3.5% ↓ in kcal from sweets for older intervention youths. |
| Weber. et al. [ ] | Review and analysis of features | WIC participants | 17 app features | Organizational and community | -Reviewing app stores and their benefits to users. | App features were classified into categories for shopping management, WIC required nutrition education modules and others. The app was rated with 4–5/5 stars |
| White et al. [ ] | Multicenter randomized intervention trial | Children | 53 | Community and policy | -Increasing food access based on availability, accessibility, affordability, acceptability, and accommodation. | Availability was enhanced for those who could select their own produce items. Flexible pick-up times and locations. ↑ access to F&V. |
| McGuirt et al. [ ] | Qualitative Study | Women of child-bearing age | 37 | Individual, organizational, and policy | -Examine willingness to shop at farmers’ markets. | More likely to shop at farmers’ market when price saving ↑ at least 20%. |
↑ indicates increase, ↓ indicates reduction.

Multilevel approaches to increase healthy food consumption in low-income populations, based on the SEM [ 36 ].
Adding culturally competent aspects to a community approach, with resources focused on multiethnic communities, materials provided in the population’s native language, and incorporation of recipes and food demonstrations from their country of origin, may result in improvements in diet quality [ 38 ]. Hammons et al. [ 38 ] added these cultural aspects and reported greater interest for the individuals to try recipes provided with fruits and vegetables and an overall increase in daily servings of fruits and vegetables consumed [ 38 ]. The results are supported by another study that reported an increase in variety of fruits and vegetables ( p < 0.01 for both), after a six-week cooking program at the Community Food Bank that teaches food pantry clients plant-based recipes [ 39 ]. These data further indicated a decrease in purchases of carbonated beverages and desserts with a value of p < 0.01 [ 39 ].
B’more Healthy Communities for Kids was a multilevel obesity prevention study that sought to improve healthier food purchasing and help reduce sweet-snack consumption among low-income African-American youths [ 40 ]. This group worked to achieve the objectives for two-year time period, through youth-led nutrition education in recreation centers, in-store promotion, and social media programs [ 40 ]. In this multilevel approach, many areas for education were considered, including promoting healthier alternatives to beverages and snacks, and sharing information for healthier cooking methods through promoting healthier cooking ingredients, such as low-fat milk, 100% whole wheat bread, and fresh/canned/frozen vegetables [ 40 ]. The multiple components involved wholesales, which were encouraged to stock B’more Healthy Communities for Kids-promoted healthier food alternatives [ 40 ]. They also worked on improving supply for healthier options of foods and beverages in corner stores and carryout restaurants, as well as improving demand through taste tests for healthier alternatives [ 40 ]. Posters, handouts, and educational sessions were provided. Through these sessions there were peer-led, hands-on activities where participants learned different sugar and fat contents in drinks and snacks and were introduced to the traffic light labeling method for beverages and snacks [ 40 ]. For additional resources, recipes, news, and educational activities related to healthier eating behaviors were sent through social media and texting [ 40 ]. The text message platform was focused towards caregivers with goal setting strategies and educational activities, where they received messages three to five times a week related to healthier eating behavior [ 40 ].
B’more Healthy Communities for Kids also worked with key city stakeholders to support policies for a healthier food environment and provided evidence-based information to support the development of policies at the city level using a Geographic Information System/System Science simulation model to help stakeholder decision-making in regard to sugar-sweetened beverage warning labels, urban farm tax credits, mobile meals, etc. [ 40 ]. The results showed that the overall intervention group purchased 1.4 more healthier foods and beverages per week in relation to the comparison youth. Additionally, there was a decrease in calorie intake from sweet snacks and desserts among older intervention youths [ 40 ]. This finding was supported by other results in improving the availability of healthier foods and beverages in small food stores in intervention zones, indicating that food availability affects an individual’s choice [ 40 ]. Overweight and obesity are major issues, especially in low-income communities, but community-enhanced school programs can be effective in reducing childhood obesity in these populations [ 41 ]. Schools with health program training and community partnerships decreased the percentage of students classified as overweight/obese by 8.3%, compared to a 1.3% decrease in schools that were provided only with health program training, without the community aspect [ 41 ].
In the case of emergency food aid, there are also food banks open and available around the US. Wetherill et al. [ 42 ] conducted a study to look a strategies and innovative programs that are focused on advancing nutrition-focused food banking in the United States. This study included in-person or phone interviews to obtain further information regarding personal experiences, perceptions, and practices related to nutrition-focused food banking [ 42 ]. Overall, the study findings indicated that food banks are implementing a variety of multi-level approaches to improve healthy food access among users [ 42 ]. This is done through four major themes: building a healthier food inventory at the food bank; enhancing partner agency healthy food access, storage, and distribution capacity; nutrition education outreach; and expanding community partnerships and intervention settings for healthy food distribution, including healthcare and schools [ 42 ].
5.1. Individual Nutrition Education and Peer Education
The main factors that have been shown to increase fruit and vegetable consumption in multilevel approaches are taste tests and nutrition education, including providing healthy recipes for participants [ 37 ]. Along with healthy recipes, some studies have focused on helping improve participants’ cooking skills to make low-cost meals, which further decreased food insecurity, by increasing cooking at home and reducing the amount of time people ate out at restaurants, leading to increased total variety of vegetables and fruits in the diet [ 34 , 37 , 39 , 40 ]. Even short-term nutrition education has made people more aware concerning sodium in processed foods and nutrient and calorie-dense foods, the importance of physical activity, and interpreting nutrition levels [ 43 ].
WIC focuses on improving the health and nutritional status of pregnant and postpartum low-income women and children up to the age of 5 years. The participants of these programs are faced with many barriers when shopping for the correct foods on their WIC food list, therefore nutrition education is a great tool to better assist this population [ 44 ]. Through mobile phone apps, there are educational tools to help the participants with shopping management features, clinic appointments, and informational resources [ 44 ]. Shopping management features assisted the WIC participants with real-time shopping for WIC foods in the grocery store, including food benefit balance checking, barcode scanning, and checking if the item was WIC eligible [ 44 ]. The participants shared that this app was very easy to use and convenient in helping pick the right products, while saving time [ 44 ]. Some applications also allowed participants to manage their WIC clinic visits, and view their future appointments and the documents needed to be provided in the appointments [ 44 ]. Required nutrition education modules were also features, which could be completed from home instead of going to the clinic [ 44 ]. Throughout a 7 month period, Weber et al. [ 44 ] reviewed the main features of a publicly available mobile phone app for WIC participants and concluded that, even though all the features were beneficial and useful, the most frequently used were the shopping management features. Some users shared their feedback, giving the app 4–5 stars out of 5 stars for being time saving, convenient, and an overall great app [ 44 ]. Other users would have liked in addition a nutrition/healthy section with recipes and ideas to help people learn to consume healthier choices, not just the WIC-approved foods [ 44 ].
Another approach to increase diet quality for low-income populations is individual tailoring of nutrition education [ 18 ]. A recent pilot 8 week study assessed the effectiveness and acceptability of personalized nutrition intervention for mobile food pantry users [ 45 ]. When comparing the treatment group with the control group, a personalized nutrition education intervention was effective in improving the diet for food-insecure participants (4.54% vs. 0.18% improvement in healthy eating index scores) [ 45 ]. Culturally tailored nutrition education involving family time and physical activity has also been a way to incorporate healthier food choices [ 46 , 47 ]. These approaches also include educational information in the participant’s native language, including all the handouts, recipes, and visual guides [ 47 ]. Focusing on diet based on culture, studies have also worked with tiendas, small Latino stores, to promote greater intake of fresh produce among consumers [ 46 ].
Education programs culturally tailored to a specific group have also been shown to be effective. Flores-Luevano et al. [ 48 ] conducted a bilingual culturally tailored, hands-on diabetes education program among Mexican American adults with diabetes. The sessions were interactive with demonstrations, activities to promote problem-solving, and facilitated group dynamics through sharing personal experiences [ 48 ]. This, intertwined with peer-education, resulted in improvements in glycated hemoglobin by −1.1% and total cholesterol with −17.2 mg/dL at 6 months post-intervention [ 48 ]. There were also behavioral changes, such as glucose self-monitoring improvement by 1.3 times increase a week, increased exercise levels, and increased positive nutritional behavior by 2.23, and the benefits were observed with attendance rates as low as 50% [ 48 ].
Marshall et al. [ 49 ] conducted a two-year follow-up study using a one-group pre-post evaluation design that focused on school-based nutrition education and food co-op intervention and how it can increase children’s intake of fruits and vegetables. In this study, 407 families completed baseline data, of which 262 parent-dyads agreed to participate in the two-year follow-up study, where the parents were provided with education along with their children [ 49 ]. This nutrition education included changes in home setting, such as increased frequency of cooking behaviors, increased usage of nutrition facts labels in making grocery purchasing decisions, and increased food availability of fruits and vegetables [ 49 ]. The results of the study showed an increase in child intake of fruits by 0.18 cup/day, vegetables by 0.14 cup/day, and fiber by 1.06 g/1000 kcal, and a significant decrease in total fat intake by 1.55 g/1000 kcal and percent daily calories from sugary beverages by 0.52% [ 49 ]. Parents also reported an increase in daily intake of vegetables by 0.6 cups/d and combined fruits and vegetables ( p < 0.05) [ 49 ].
5.2. Community-Based Participatory Research
Community-based participatory research is a kind of study where community members, organizational representatives, and academic researchers are all equally involved in the process [ 50 ]. This research method is important to collect the data on what kind of lessons and resources will be beneficial for the population, but also to make the participants more comfortable and more open when conducting interviews with educators of the community. This approach was used in the selected studies to modify elements in the environment, which would result in an increase in nutrient-dense food consumption. A number of studies have focused on improving diet quality and reducing metabolic risk through gardening and cooking [ 47 , 48 , 51 ]. These studies organized classes tailored towards low-income youths and consisted of lessons about gardening, where they used “hands-on” approaches to facilitate participation in planting, growing, and harvesting organic fruits and vegetables [ 47 , 48 , 51 ]. Additional interactive cooking and nutrition lessons were included with the fruits and vegetables raised from the garden [ 47 , 51 ].
These elements worked to increase fruit and vegetable consumption and preparation of healthy snacks and meals [ 47 , 51 ]. Creative food preparation with blending of new vegetables into juices or other dishes has also been a way to introduce unfamiliar foods to children and other family members [ 47 , 51 , 52 ]. Participants shared that their children would be curious of the new items introduced each week and they were excited to include them in their smoothies [ 47 , 51 , 52 ].
As previously mentioned, accessibility and affordability are two of the main factors that lead to food security. Since supermarkets and convenience stores are known to have expensive products, a way to provide access to food in low-income families is community-supported agriculture products. Community-supported agriculture products are more affordable and flexible in their accessibility [ 52 ]. Farm Fresh Foods for Healthy Kids examined the perception of food access among low-income families in nine communities participating in community-supported agriculture [ 52 ]. Participants reported improved access to food products and benefited from flexible pick-up times and locations; however, despite the cost being relatively low, payment remained a barrier for some [ 52 ]. A multistate randomized intervention trial targeted obesity prevention in low-income families through improving access to affordable, local, seasonal produce through community-supported agriculture and support of obesity-related behavior changes through tailored education to increase knowledge and skills, and provide increased revenue and business to support community-supported agriculture farmers [ 53 ]. Even though the community took steps to help low-income populations, there are still barriers that need to be faced for more effective results of current and future studies [ 53 ]. When shopping through community-supported agriculture, participants believed that they were saving money for produce of high quality, compared to the grocery stores [ 53 ].
McGuirt et al. [ 54 ] examined the influence of farmers’ market pricing and accessibility on willingness to shop at farmers’ markets, among low-income women. Percentage price savings were presented visually as discounts at the standard amount, or there were pictures of the amount of produce a consumer could buy at the farmers’ market compared to the supermarket, reflecting the savings [ 54 ]. The different quantity bought with the same price was determined by a member of the research group who went to local supermarkets to establish the price per pound and calculate the amount to compare with the products from the farmers’ market [ 54 ]. The results of this study showed that there was an increased interest to shop at farmers’ markets when there was at least a 20% price saving [ 54 , 55 ]. Additionally, participants were more influenced by the visual representation of a greater quantity of produce with the price savings, rather than the money saved by the reduced price [ 54 ].
5.3. Policy Changes in Supplemental Nutrition Programs
To reduce energy-dense, low-nutrient food consumption, there need to be environmental and policy changes that promote healthy eating. The main categories that need to be in focus, based on research, are pricing, nutrition labeling, and access to healthier ready-to-go foods [ 55 , 56 , 57 ]. Additionally, to increase food security and diet quality, policy changes are needed in school programs that work on strengthening links to the traditional, nutrient-dense food system in schools [ 58 ]. A significant increase in fruit and vegetable intake has been shown with greater access to healthier ready-to-go foods [ 58 ]. Additionally, reducing the cost of healthier snacks increases the consumption of these products [ 57 , 59 ]. When prices of fruits and vegetables were reduced by 50% for high school students, their consumption increased by twofold to fourfold [ 55 ]. Low-fat snack sales increased by 93% with a 50% reduction in their prices [ 59 ]. Studies also worked with key city stakeholders to support policies for a healthier food environment and provided evidence-based information to support the development of these policies [ 40 ].
6. Discussion and Conclusions
Food insecurity is a widespread problem in the US that greatly affects quality of life, leading to greater risk for obesity, diabetes, and cardiovascular diseases. There are a number of barriers causing food insecurity in certain areas, such as lack of transportation, food deserts or food swamps, and lack of nutrition education. This review paper discussed certain approaches to reduce food insecurity in low-income communities and increase access to healthful foods, especially consumption of fruits and vegetables. Multilevel approaches are shown to have the most distinguishable results and also take into consideration a wide spectrum of reasons and factors. Multilevel approaches have included nutrition educational material, taste-testing events, price reduction of healthy products, increased access to healthy options, and overall policy changes. The major limitation to multilevel approaches is that when a change is observed, there is not a way to specifically identify which components of the intervention led to changes in food behaviors [ 35 ]. Other potential limitations of studies thus far have included small sample sizes and sample populations that were predominantly women, self-reporting of data, potentially leading to bias, and the possibility that participants may not have fully represented the low-income population of interest [ 38 , 39 , 53 , 55 ]. Beneficial approaches comprise community-based research, which obtains an input from the community, where the main focus is on factors that lead to food insecurity and how to reduce these barriers. Farmers’ markets that provide local, seasonal, affordable produce are shown to be a way to support behavior changes and increase access to fresh produce [ 12 ]. Nutrition education helps decrease food insecurity from a different approach, through hands-on activities and peer-education to increase cooking skills and help incorporate a variety of fruits and vegetables in the diet [ 17 , 37 , 49 ].
Additionally, current studies have shown a need for more research, but it is important to point out that perception of an individual’s food environment may impact the foods they purchase and consume [ 60 ]. For example, if they perceive the environment to be poor, they may be less likely to buy fruits and vegetables and other healthy options [ 60 ]. Furthermore, future research can further focus on how to effectively improve diet quality and reduce diet-related chronic disease risk by developing and validating multi-dimensional intervention studies tailored for target populations with special needs and barriers, and studying the impact of the perceived food environment and social support on improving the diet quality of a population with poor access to healthy foods.
Funding Statement
This research received no external funding.
Author Contributions
Conceptualization, D.Z., O.K.C. and M.J.P.; writing—original draft preparation, D.Z.; writing—review and editing, D.Z., O.K.C. and M.J.P. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Informed consent statement, data availability statement, conflicts of interest.
The authors declare no conflict of interest.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
IMAGES
VIDEO
COMMENTS
The impact of food insecurity on health outcomes: empirical ...
Food insecurity is now recognized as a major health crisis in the United States. This is due to the size of the problem—more than 42 million persons were food insecure in 2015—as well as the multiple negative health outcomes and higher health care costs attributable to food insecurity.
Food Insecurity and Child Development: A State-of-the-Art ...
prevalence of severe food insecurity was 10.2% in 2017, affecting 770 million people. Food insecurity and. malnutrition are caused by unequal and unjust distribution of nourishing food due to ...
For more information, contact: Alisha Coleman-Jensen, Matthew P. Rabbitt, Christian A. Gregory, and Anita Singh. In 2021, 10.2 percent (13.5 million) of U.S. households were food insecure, meaning they had difficulty at some time during the year providing enough food for all their members because of a lack of resources.
Food insecurity has economic root causes
Attributing changes in food insecurity to a changing climate
Food insecurity is prevalent, affecting 1·2 billion people globally in 2021. However, the effects of food insecurity are unequally distributed across populations and climate-related shocks threaten to exacerbate food insecurity and associated health consequences. The mechanisms underlying this exacerbation at the household level are largely unknown. We aimed to synthesise the available ...
Food insecurity, the limited availability of or access to nutritionally adequate and safe foods, is a persistent health concern in the United States. 1, 2 Food insecurity disproportionately affects households with children, households headed by a single parent, and Black and Hispanic households. 1 As a result of the ongoing coronavirus disease 2019 pandemic, a recent report showed that food ...
World Food Day — 16 October, with the theme this year of 'leave no one behind' — is an appropriate time to reflect on global progress toward Sustainable Development Goal 2: Zero Hunger.
1. Introduction. Food security (FS) is "a situation that exists when all people, at all times, have physical, social and economic access to sufficient, safe and nutritious food that meets their dietary needs and food preferences for an active and healthy life" [] p.3.It is a significant priority for international policy [], and has been perceived as being among the key challenges worldwide ...
This impact is higher in the case of moderate to severe food insecurity, with a 1 ∘C increase in temperature anomaly resulting in a 1.58% (95% CI 1.48-1.68) increase in 2014 but a 2.14% (95% CI 2.08-2.20) increase in 2019. Thus, the results show that the temperature anomaly has not only increased the probability of food insecurity, but ...
Food Insecurity And Health Outcomes
Food insecurity and the lack of access to affordable, nutritious food are associated with poor dietary quality and an increased risk of diet-related diseases, including cardiovascular disease, diabetes, and certain types of cancer. Those of lower socioeconomic status and racial and ethnic minority groups experience higher rates of food insecurity, are more likely to live in under-resourced ...
Research priorities for global food security under extreme ...
Food insecurity is an economic condition m, eaning that it is driven primarily by lack of money ... We think the following conditions have a relationship with food insecurity, but a dditional research is needed. High healthcare costs (e.g., chronic, pre-existing conditions , reliance on medication) and
Policies to reduce food insecurity: An ethical imperative
Research Working Paper Series 4703. Collier, P. (2007) ... Food insecurity problems still exist among people in low-to-middle income countries. The long-term disadvantages of socioeconomic status ...
Food insecurity affects all communities worldwide as many find it difficult to consistently access nutritious, affordable food. This problem is exacerbated by conflict, political insecurity, climate change, and global shocks such as the COVID-19 pandemic. This Special Issue seeks to develop a collection of innovative, contemporary research that ...
Food Insecurity: Concept, Causes, Effects and Possible ...
Furthermore, much of the current research has been performed in the United States, and experiences of food insecurity may be different in Canada. In addition, there is a lack of research examining vulnerable groups, such as First Nations populations, who have unique food security considerations related to traditional food practices ( 4 ).
Increasing Access to Healthy Foods through Improving ...